Effects of a New York Medicaid Care Management Program on Substance Use Disorder Treatment Services and Medicaid Spending: Implications for Defining the Target Population.
Charles J Neighbors, Rajeev Yerneni, Yi Sun, Sugy Choi, Constance Burke, Megan A O'Grady, Rebecca McDonald, Jon Morgenstern
{"title":"Effects of a New York Medicaid Care Management Program on Substance Use Disorder Treatment Services and Medicaid Spending: Implications for Defining the Target Population.","authors":"Charles J Neighbors, Rajeev Yerneni, Yi Sun, Sugy Choi, Constance Burke, Megan A O'Grady, Rebecca McDonald, Jon Morgenstern","doi":"10.1177/11782218221075041","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>We examined the effects of a statewide New York (NY) care management (CM) program for substance use disorder (SUD), Managed Addiction Treatment Services (MATS), on SUD treatment services' utilization and spending among patients with a recent history of high Medicaid spending and among those for whom a predictive algorithm indicates a higher probability of outlier spending in the following year.</p><p><strong>Methods: </strong>We applied difference-in-difference analyses with propensity score matching using NY Medicaid claims data and a state registry of SUD-treatment episodes from 2006 to 2009. A total of 1263 CM enrollees with high SUD treatment spending (>$10K) in the prior year and a matched comparison group were included in the analysis. Crisis care utilization for SUD (detoxification and hospitalizations), outpatient SUD treatment, and Medicaid spending were examined over 12 months among both groups. CM effects among predicted high-future-spending patients (HFS) were also analyzed.</p><p><strong>Results: </strong>CM increased outpatient SUD treatment visits by approximately 10.5 days (95% CI = 0.9, 20.0). CM crisis care and spending outcomes were not statistically different from comparison since both conditions had comparable pre-post declines. Conversely, CM significantly reduced SUD treatment spending by approximately $955 (95% CI = -1518, -391) and reduced days of detox utilization by about 1.0 days (95% CI = -1.9, -0.1) among HFS.</p><p><strong>Conclusion: </strong>Findings suggest that CM can reduce SUD treatment spending and utilization when targeted at patients with a greater likelihood of high future spending, indicating the potential value of predictive models to select CM patients.</p>","PeriodicalId":22185,"journal":{"name":"Substance Abuse: Research and Treatment","volume":" ","pages":"11782218221075041"},"PeriodicalIF":2.4000,"publicationDate":"2022-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/d9/9a/10.1177_11782218221075041.PMC8808013.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Substance Abuse: Research and Treatment","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11782218221075041","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
引用次数: 0
Abstract
Aims: We examined the effects of a statewide New York (NY) care management (CM) program for substance use disorder (SUD), Managed Addiction Treatment Services (MATS), on SUD treatment services' utilization and spending among patients with a recent history of high Medicaid spending and among those for whom a predictive algorithm indicates a higher probability of outlier spending in the following year.
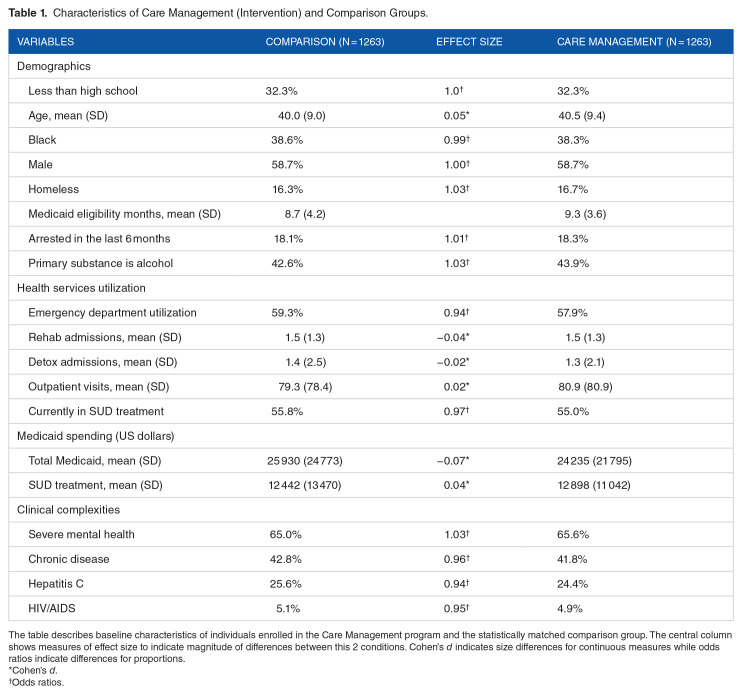
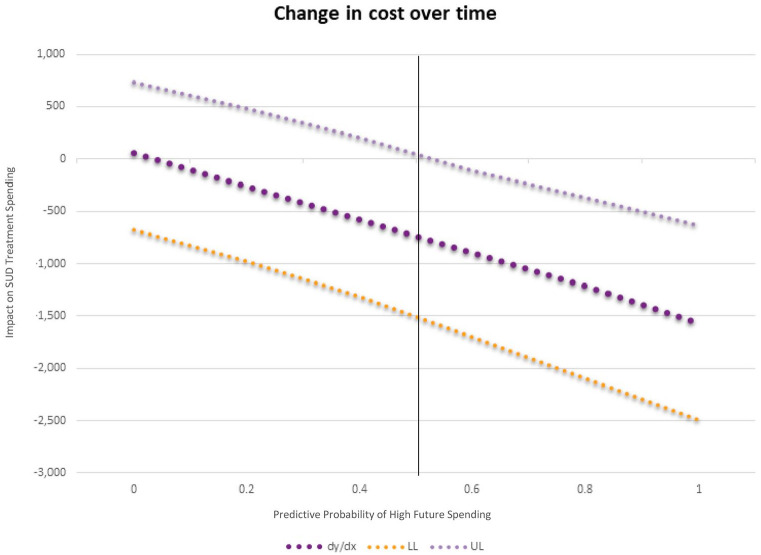
Methods: We applied difference-in-difference analyses with propensity score matching using NY Medicaid claims data and a state registry of SUD-treatment episodes from 2006 to 2009. A total of 1263 CM enrollees with high SUD treatment spending (>$10K) in the prior year and a matched comparison group were included in the analysis. Crisis care utilization for SUD (detoxification and hospitalizations), outpatient SUD treatment, and Medicaid spending were examined over 12 months among both groups. CM effects among predicted high-future-spending patients (HFS) were also analyzed.
Results: CM increased outpatient SUD treatment visits by approximately 10.5 days (95% CI = 0.9, 20.0). CM crisis care and spending outcomes were not statistically different from comparison since both conditions had comparable pre-post declines. Conversely, CM significantly reduced SUD treatment spending by approximately $955 (95% CI = -1518, -391) and reduced days of detox utilization by about 1.0 days (95% CI = -1.9, -0.1) among HFS.
Conclusion: Findings suggest that CM can reduce SUD treatment spending and utilization when targeted at patients with a greater likelihood of high future spending, indicating the potential value of predictive models to select CM patients.
目的:我们研究了纽约州(NY)药物使用障碍(SUD)的护理管理(CM)计划,管理成瘾治疗服务(MATS)对近期有高医疗补助支出史的患者以及预测算法表明次年异常支出概率较高的患者的SUD治疗服务的利用和支出的影响。方法:我们使用纽约州医疗补助索赔数据和2006年至2009年的sud治疗事件的州登记处,采用倾向评分匹配的差异分析。分析共纳入了1263名前一年患有高SUD治疗费用(> 1万美元)的CM患者和匹配的对照组。对两组患者在12个月内对SUD的危机护理利用(戒毒和住院治疗)、门诊SUD治疗和医疗补助支出进行了检查。预测的高未来消费患者(HFS)的CM效应也进行了分析。结果:CM增加了约10.5天的门诊SUD治疗次数(95% CI = 0.9, 20.0)。CM危机护理和支出结果与比较没有统计学差异,因为两种情况都有可比的前后下降。相反,在HFS中,CM显着减少了约955美元的SUD治疗费用(95% CI = -1518, -391),并减少了约1.0天的排毒利用天数(95% CI = -1.9, -0.1)。结论:研究结果表明,当CM针对未来高支出可能性较大的患者时,CM可以减少SUD治疗支出和利用率,这表明预测模型在选择CM患者方面具有潜在价值。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


