{"title":"Minimally Invasive Successful Reconstruction of a Severely Traumatized Upper Extremity Using Platelet-Rich Plasma and Tissue Scaffold: A Case Report.","authors":"Srinjoy Saha","doi":"10.1055/s-0041-1742176","DOIUrl":null,"url":null,"abstract":"<p><p>Minimally invasive reconstruction combines principles of tissue engineering and regenerative medicine for healing complex wounds. This approach was successfully demonstrated on a 64-year-old diabetic and hypertensive male patient, who was brought unconscious to our emergency after surviving an automobile collision with severe brain and right-dominant upper extremity injuries. Uncontrolled hyperglycemia, severe anemia, diffuse axonal brain injury, wrist drop, and loss of thumb extension and abduction were noted. Extensive degloving, skin necrosis, extensor and flexor forearm muscle crush injuries, and ruptured extensor tendons were observed. Serial wound debridement combined with platelet-poor plasma injection into the muscles, platelet-rich plasma injections into the tendons and subcutis, and low-negative pressure wound therapy were performed sequentially to salvage the injured soft-tissues. Improvements were noticed during the second exploration after 5 days. Surviving muscles showed adequate vascularization and revival of innervation during the third exploration after another 5 days. Thereafter, absorbable synthetic tissue scaffold was applied over a sizeable 270 cm <sup>2</sup> wound as a flap-alternative. Tissues regenerated well within the scaffold during the next 2 months, halving the wound area to 132 cm <sup>2</sup> . A thick split-skin graft was applied over the remaining granulating neodermis, which \"took\" completely. Six months postoperatively, the patient regained most hand functions and performed all activities satisfactorily, while the grafted area appeared almost identical to surroundings. Minimally invasive reconstruction thus produced satisfying results with fewer shorter simpler surgeries, minimal anesthesia, short-duration hospitalization, lower health care costs, lesser risks, and excellent patient-reported outcomes.</p>","PeriodicalId":44614,"journal":{"name":"Surgery Journal","volume":" ","pages":"e28-e33"},"PeriodicalIF":0.8000,"publicationDate":"2022-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8763461/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0041-1742176","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 3
Abstract
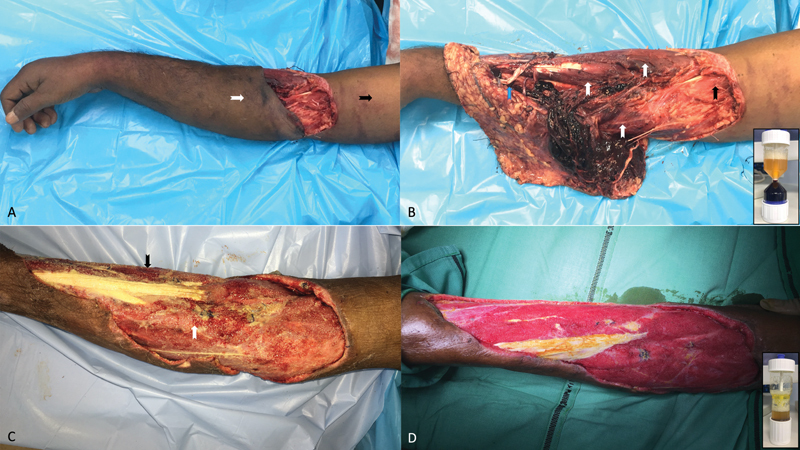
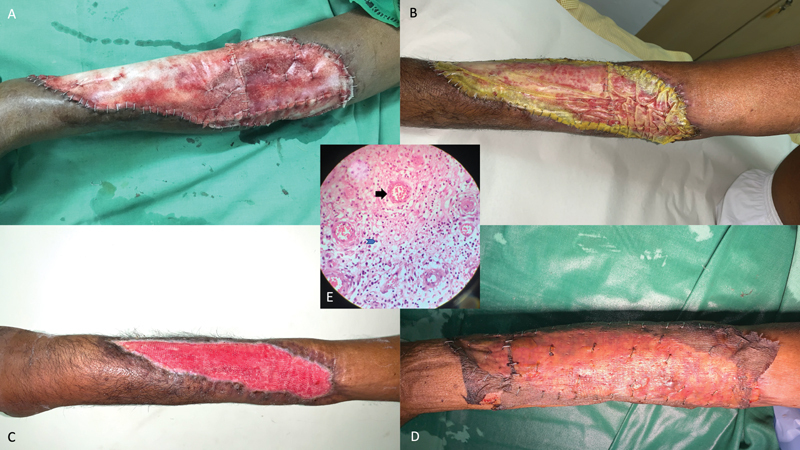
Minimally invasive reconstruction combines principles of tissue engineering and regenerative medicine for healing complex wounds. This approach was successfully demonstrated on a 64-year-old diabetic and hypertensive male patient, who was brought unconscious to our emergency after surviving an automobile collision with severe brain and right-dominant upper extremity injuries. Uncontrolled hyperglycemia, severe anemia, diffuse axonal brain injury, wrist drop, and loss of thumb extension and abduction were noted. Extensive degloving, skin necrosis, extensor and flexor forearm muscle crush injuries, and ruptured extensor tendons were observed. Serial wound debridement combined with platelet-poor plasma injection into the muscles, platelet-rich plasma injections into the tendons and subcutis, and low-negative pressure wound therapy were performed sequentially to salvage the injured soft-tissues. Improvements were noticed during the second exploration after 5 days. Surviving muscles showed adequate vascularization and revival of innervation during the third exploration after another 5 days. Thereafter, absorbable synthetic tissue scaffold was applied over a sizeable 270 cm 2 wound as a flap-alternative. Tissues regenerated well within the scaffold during the next 2 months, halving the wound area to 132 cm 2 . A thick split-skin graft was applied over the remaining granulating neodermis, which "took" completely. Six months postoperatively, the patient regained most hand functions and performed all activities satisfactorily, while the grafted area appeared almost identical to surroundings. Minimally invasive reconstruction thus produced satisfying results with fewer shorter simpler surgeries, minimal anesthesia, short-duration hospitalization, lower health care costs, lesser risks, and excellent patient-reported outcomes.
微创重建结合了组织工程和再生医学的原理,用于治疗复杂的伤口。该方法在一名64岁的糖尿病和高血压男性患者身上得到了成功的证明,该患者在一次汽车碰撞中幸存下来,并伴有严重的脑部和右上肢损伤,随后被送往我们的急诊室。未控制的高血糖,严重贫血,弥漫性脑轴索损伤,手腕下垂,拇指伸展和外展丧失。大面积脱手套,皮肤坏死,前臂伸肌和屈肌挤压损伤,伸肌腱断裂。采用连续创面清创联合贫血小板血浆肌内注射、富血小板血浆肌腱及皮下注射、低负压创面治疗,抢救损伤软组织。在5天后的第二次探测中发现了改善。存活的肌肉在5天后的第三次探查中显示出充足的血管化和神经支配的恢复。此后,可吸收的合成组织支架应用于一个相当大的270 cm 2伤口作为皮瓣替代。在接下来的2个月里,组织在支架内再生良好,伤口面积减半至132平方厘米。将厚的裂皮移植物应用于剩余的肉芽状新生真皮,使其完全“吸收”。术后6个月,患者大部分手部功能恢复,活动满意,移植区与周围环境基本一致。因此,微创重建以更少、更简单的手术、最少的麻醉、较短的住院时间、较低的医疗费用、较小的风险和良好的患者报告结果产生了令人满意的结果。


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


