Tosan Okoro, Sebastian Tomescu, J Michael Paterson, Bheeshma Ravi
{"title":"Analysis of the relationship between surgeon procedure volume and complications after total knee arthroplasty using a propensity-matched cohort study.","authors":"Tosan Okoro, Sebastian Tomescu, J Michael Paterson, Bheeshma Ravi","doi":"10.1136/bmjsit-2020-000072","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>This study aimed to identify a threshold in annual surgeon volume associated with increased risk of revision (for any cause) and deep infection requiring surgery following primary elective total knee arthroplasty (TKA).</p><p><strong>Design: </strong>A propensity score matched cohort study.</p><p><strong>Setting: </strong>Ontario, Canada.</p><p><strong>Participants: </strong>169 713 persons who received a primary TKA between 2002 and 2016, with 3-year postoperative follow-up.</p><p><strong>Main outcome measures: </strong>Revision arthroplasty (for any cause), and the occurrence of deep surgical infection requiring surgery.</p><p><strong>Results: </strong>Based on restricted cubic spline analysis, the threshold for increased probability of revision and deep infection requiring surgery was <70 cases/year. After matching of 51 658 TKA recipients from surgeons performing <70 cases/year to TKA recipients from surgeons with greater than 70 cases/year, patients in the former group had a higher rate of revision (for any cause, 2.23% (95% Confidence Interval (CI) 1.39 to 3.07) vs 1.70% (95% CI 0.85 to 2.55); Hazard Ratio (HR) 1.33, 95% CI 1.21 to 1.47, p<0.0001) and deep infection requiring surgery (1.29% (95% CI 0.44 to 2.14) vs 1.09% (95% CI 0.24 to 1.94); HR 1.33, 95% CI 1.17 to 1.51, p<0.0001).</p><p><strong>Conclusions: </strong>For primary TKA recipients, cases performed by surgeons who had performed fewer than 70 TKAs in the year prior to the index TKA were at 31% increased relative risk of revision (for any cause), and 18% increased relative risk for deep surgical infection requiring surgery, at 3-year follow-up.</p>","PeriodicalId":33349,"journal":{"name":"BMJ Surgery Interventions Health Technologies","volume":"3 1","pages":"e000072"},"PeriodicalIF":2.1000,"publicationDate":"2021-04-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/bmjsit-2020-000072","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Surgery Interventions Health Technologies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjsit-2020-000072","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 8
Abstract
Objectives: This study aimed to identify a threshold in annual surgeon volume associated with increased risk of revision (for any cause) and deep infection requiring surgery following primary elective total knee arthroplasty (TKA).
Design: A propensity score matched cohort study.
Setting: Ontario, Canada.
Participants: 169 713 persons who received a primary TKA between 2002 and 2016, with 3-year postoperative follow-up.
Main outcome measures: Revision arthroplasty (for any cause), and the occurrence of deep surgical infection requiring surgery.
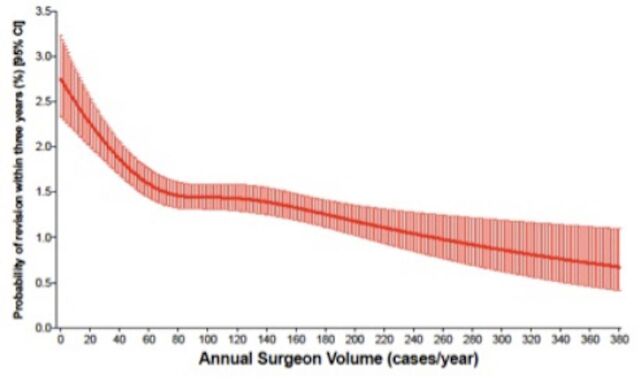
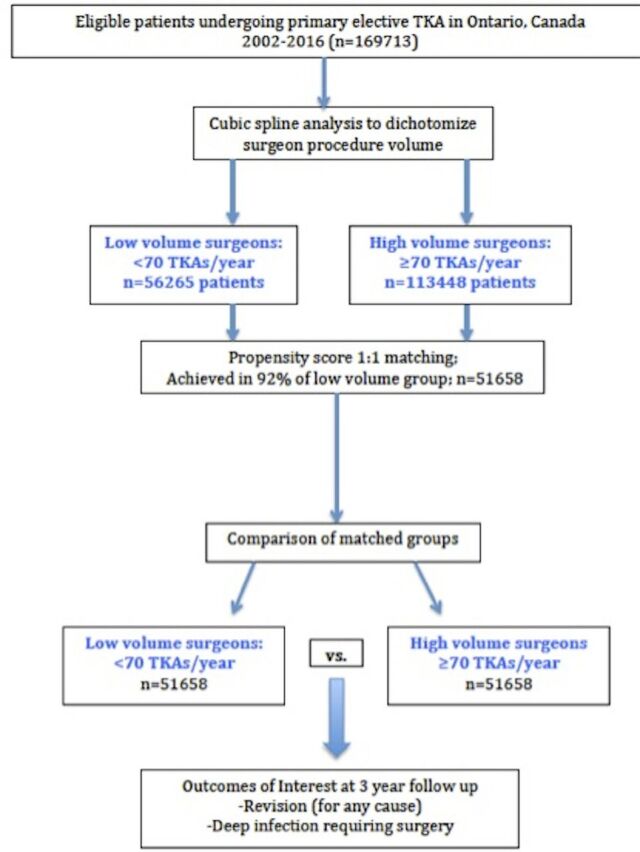
Results: Based on restricted cubic spline analysis, the threshold for increased probability of revision and deep infection requiring surgery was <70 cases/year. After matching of 51 658 TKA recipients from surgeons performing <70 cases/year to TKA recipients from surgeons with greater than 70 cases/year, patients in the former group had a higher rate of revision (for any cause, 2.23% (95% Confidence Interval (CI) 1.39 to 3.07) vs 1.70% (95% CI 0.85 to 2.55); Hazard Ratio (HR) 1.33, 95% CI 1.21 to 1.47, p<0.0001) and deep infection requiring surgery (1.29% (95% CI 0.44 to 2.14) vs 1.09% (95% CI 0.24 to 1.94); HR 1.33, 95% CI 1.17 to 1.51, p<0.0001).
Conclusions: For primary TKA recipients, cases performed by surgeons who had performed fewer than 70 TKAs in the year prior to the index TKA were at 31% increased relative risk of revision (for any cause), and 18% increased relative risk for deep surgical infection requiring surgery, at 3-year follow-up.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


