{"title":"Risk Benefit Analysis of Routine Thymectomy for Differentiated Thyroid Cancers: A Systematic Review.","authors":"Pallvi Kaul, Priyanka Kaul, Dharma Ram Poonia, Ashish Jakhetiya, Vipin Arora, Pankaj Kumar Garg","doi":"10.1055/s-0041-1736669","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background</b> Central compartment lymph node dissection (CLND) is a part of the surgical management of differentiated thyroid cancer (DTC). Therapeutic CLND is done to address clinically significant central compartment nodes in patients with DTC, while prophylactic CLND is performed in the presence of high-risk features in the absence of clinically significant neck nodes. Removal of thymus-unilateral or bilateral-during CLND to achieve complete clearance of level VI and VII lymph node stations and address thymic metastasis is debatable. <b>Objective</b> The present systematic review was conducted to summarize the evidence, delineating the role of thymectomy during CLND in patients with DTC. <b>Methods</b> Electronic databases of PubMed, Embase, and Cochrane were searched from their inception to July 2020 using keywords-thyroid neoplasms or tumors, thyroidectomy, and thymectomy-to identify the articles describing the role of thymectomy during CLND in DTC. A pooled analysis of surgicopathological outcomes was performed using metaprop command in STATA software version 16. <b>Result</b> A total of three studies and 347 patients-total thyroidectomy (TT) with bilateral thymectomy in 154, TT with unilateral thymectomy in 166, and TT alone in 27 patients with DTC-were included in the systematic review. The pooled frequency of thymic metastasis was a mere 2% in patients undergoing either unilateral or bilateral thymectomy. The routine addition of thymectomy does not result in better lymph node clearance. Unilateral and bilateral thymectomy were associated with high chances of transient hypocalcemia (12.0% and 56.1%, respectively). <b>Conclusion</b> Routine thymectomy is not warranted during CLND, considering minimal oncological benefit and high risk of postoperative hypocalcemia.</p>","PeriodicalId":44614,"journal":{"name":"Surgery Journal","volume":"7 4","pages":"e307-e313"},"PeriodicalIF":0.8000,"publicationDate":"2021-12-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8674089/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Surgery Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1055/s-0041-1736669","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/10/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 2
Abstract
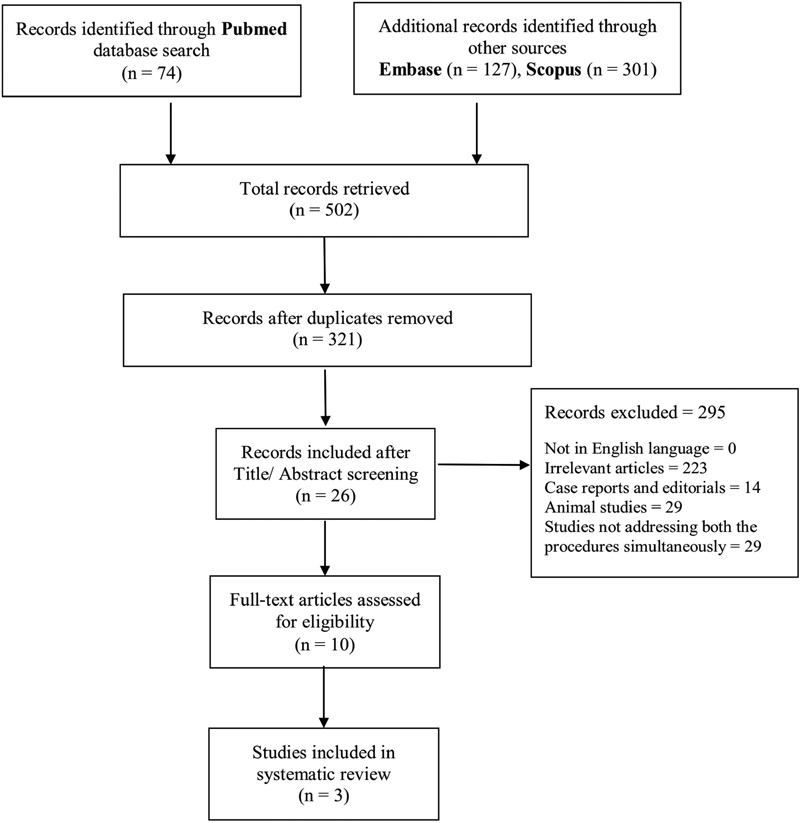
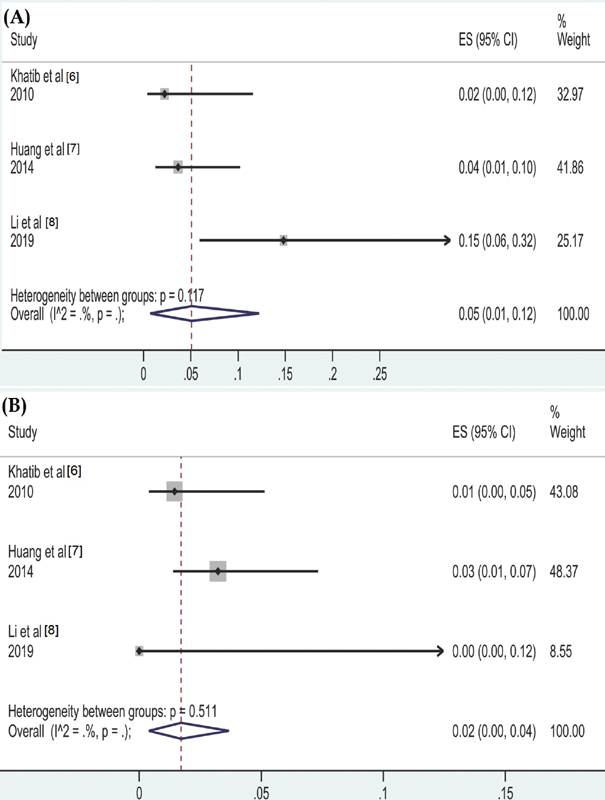
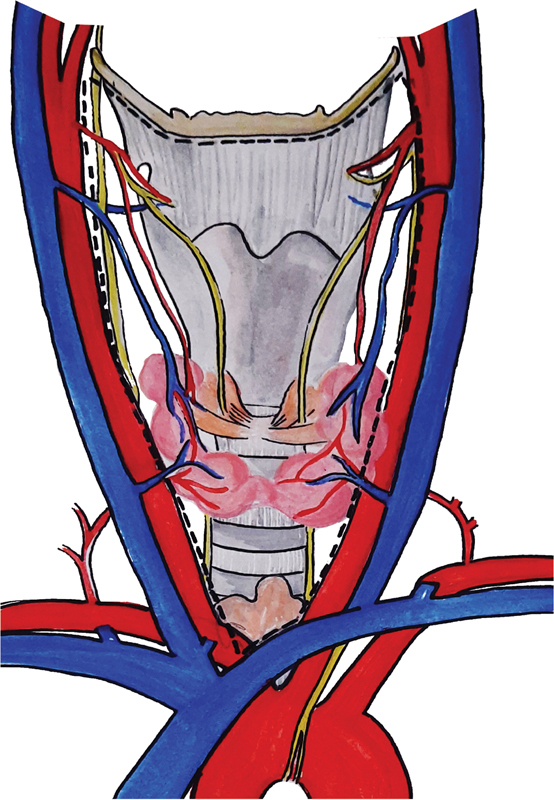
Background Central compartment lymph node dissection (CLND) is a part of the surgical management of differentiated thyroid cancer (DTC). Therapeutic CLND is done to address clinically significant central compartment nodes in patients with DTC, while prophylactic CLND is performed in the presence of high-risk features in the absence of clinically significant neck nodes. Removal of thymus-unilateral or bilateral-during CLND to achieve complete clearance of level VI and VII lymph node stations and address thymic metastasis is debatable. Objective The present systematic review was conducted to summarize the evidence, delineating the role of thymectomy during CLND in patients with DTC. Methods Electronic databases of PubMed, Embase, and Cochrane were searched from their inception to July 2020 using keywords-thyroid neoplasms or tumors, thyroidectomy, and thymectomy-to identify the articles describing the role of thymectomy during CLND in DTC. A pooled analysis of surgicopathological outcomes was performed using metaprop command in STATA software version 16. Result A total of three studies and 347 patients-total thyroidectomy (TT) with bilateral thymectomy in 154, TT with unilateral thymectomy in 166, and TT alone in 27 patients with DTC-were included in the systematic review. The pooled frequency of thymic metastasis was a mere 2% in patients undergoing either unilateral or bilateral thymectomy. The routine addition of thymectomy does not result in better lymph node clearance. Unilateral and bilateral thymectomy were associated with high chances of transient hypocalcemia (12.0% and 56.1%, respectively). Conclusion Routine thymectomy is not warranted during CLND, considering minimal oncological benefit and high risk of postoperative hypocalcemia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


