{"title":"Comprehensive Pain Control Strategy in Minimally Invasive Mitral Valve Repair.","authors":"Mitsuharu Hosono, Hiroshi Yasumoto, Shintaro Kuwauchi, Yoshino Mitsunaga, Uetsuki Tomohiko, Naoki Minato, Kohei Kawazoe","doi":"10.5761/atcs.oa.21-00131","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The effect of our comprehensive strategy to reduce pain after minimally invasive mitral valve repair through a right mini-thoracotomy was assessed retrospectively.</p><p><strong>Methods: </strong>Our comprehensive strategy constituted the following: planned rib cutting to avoid rib injury, sufficient intercostal muscle division to mobilize the cut rib, limiting the number of intercostal ports, avoiding nerve entrapment, continuous extra-pleural intercostal nerve block, and regular use of oral non-steroidal anti-inflammatory drugs. We compared patients treated with this comprehensive strategy (Group S, n = 13) and patients before this strategy was implemented (Group C, n = 13). We used a numerical rating scale (NRS) as a pain scale during the first 3 days postoperatively.</p><p><strong>Results: </strong>The average NRS was significantly lower in Group S (0.82 ± 0.49) than in Group C (2.40 ± 1.46) (P <0.01). The maximum NRS was also significantly lower in Group S (3.23 ± 1.17) than in Group C (5.69 ± 2.43) (P <0.01). The number of patients using additional single-dose analgesic were significantly less in Group S (23.1%) than in Group C (84.6%) (P <0.01).</p><p><strong>Conclusion: </strong>Our comprehensive pain control strategy effectively reduced postoperative pain in minimally invasive mitral valve repair.</p>","PeriodicalId":8037,"journal":{"name":"Annals of Thoracic and Cardiovascular Surgery","volume":"28 3","pages":"180-185"},"PeriodicalIF":1.3000,"publicationDate":"2022-06-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/b8/55/atcs-28-180.PMC9209889.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Thoracic and Cardiovascular Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.5761/atcs.oa.21-00131","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/7 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 1
Abstract
Purpose: The effect of our comprehensive strategy to reduce pain after minimally invasive mitral valve repair through a right mini-thoracotomy was assessed retrospectively.
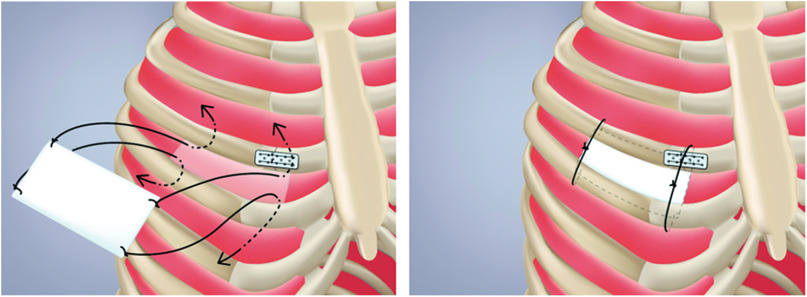
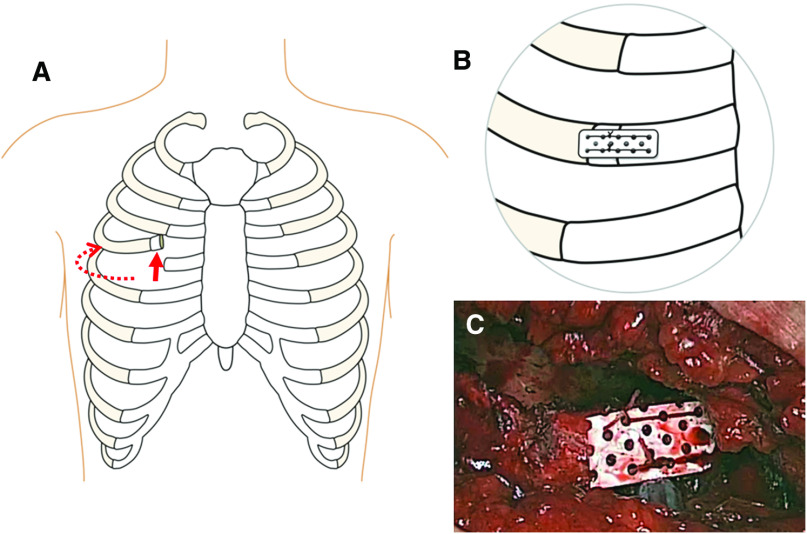
Methods: Our comprehensive strategy constituted the following: planned rib cutting to avoid rib injury, sufficient intercostal muscle division to mobilize the cut rib, limiting the number of intercostal ports, avoiding nerve entrapment, continuous extra-pleural intercostal nerve block, and regular use of oral non-steroidal anti-inflammatory drugs. We compared patients treated with this comprehensive strategy (Group S, n = 13) and patients before this strategy was implemented (Group C, n = 13). We used a numerical rating scale (NRS) as a pain scale during the first 3 days postoperatively.
Results: The average NRS was significantly lower in Group S (0.82 ± 0.49) than in Group C (2.40 ± 1.46) (P <0.01). The maximum NRS was also significantly lower in Group S (3.23 ± 1.17) than in Group C (5.69 ± 2.43) (P <0.01). The number of patients using additional single-dose analgesic were significantly less in Group S (23.1%) than in Group C (84.6%) (P <0.01).
Conclusion: Our comprehensive pain control strategy effectively reduced postoperative pain in minimally invasive mitral valve repair.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


