S Pathmanathan, S D N De Silva, M Sumanatilleke, D Lokuhetty, U V V Ranathunga
{"title":"Bilateral Leydig Cell Hyperplasia: A Rare Cause of Postmenopausal Hirsutism.","authors":"S Pathmanathan, S D N De Silva, M Sumanatilleke, D Lokuhetty, U V V Ranathunga","doi":"10.1155/2022/8804856","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Postmenopausal hirsutism could be due to a myriad of causes, including ovarian and adrenal tumours, ovarian hyperthecosis, exogenous androgens, and Cushing's syndrome. We report a patient who was found to have a rare cause of postmenopausal hirsutism. <i>Case Presentation</i>. A 64-year-old postmenopausal woman with a history of hypertension, thyrotoxicosis, and poorly controlled diabetes on multiple oral hypoglycaemic agents presented with gradual onset progressive excessive hair growth without any virilizing features. On examination, she did not have Cushingnoid features or clitoromegaly. Her hirsutism was quantified with Ferriman-Gallwey score which was 9. Her biochemical evaluation showed elevated testosterone levels with normal DHEAS, ODST, 17-OHP, and prolactin. Low-dose dexamethasone suppression test did not suppress testosterone more than 40%. Contrast-enhanced CT of the adrenal and pelvis did not show any adrenal or ovarian mass lesions. Transvaginal ultrasound scan showed bilateral prominent ovaries only. Combined adrenal and ovarian venous sampling was carried out to localize the source of excess androgen, but only the left adrenal vein was successfully cannulated which showed suppressed testosterone level compared to periphery. The patient underwent total abdominal hysterectomy and bilateral salphingo oophorectomy, and her testosterone level normalized postoperatively. Her glycaemic control improved. Histology showed evidence of bilateral diffuse ovarian Leydig cell hyperplasia.</p><p><strong>Conclusion: </strong>Evaluation of postmenopausal hirsutism needs careful history and examination followed by biochemical evaluation and imaging. While adrenal and ovarian venous sampling can help to arrive at a diagnosis, it is a technically demanding procedure with low success rates even at centers of excellence. Therefore, in such situations, bilateral oophorectomy may be the best course of action which will give the histological confirmation of the diagnosis. Successful treatment of hyperandrogenism can result in improvement of glycaemic control. Bilateral diffuse Leydig cell hyperplasia is a rare but important cause of postmenopausal hirsutism.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":" ","pages":"8804856"},"PeriodicalIF":0.9000,"publicationDate":"2022-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8858062/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/2022/8804856","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 1
Abstract
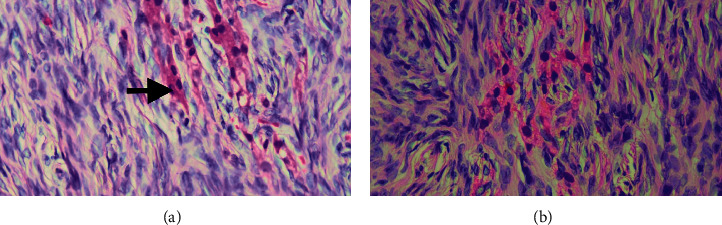
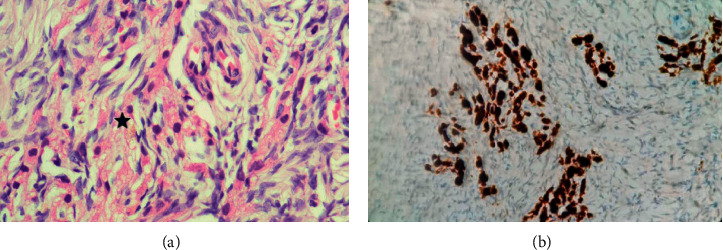
Background: Postmenopausal hirsutism could be due to a myriad of causes, including ovarian and adrenal tumours, ovarian hyperthecosis, exogenous androgens, and Cushing's syndrome. We report a patient who was found to have a rare cause of postmenopausal hirsutism. Case Presentation. A 64-year-old postmenopausal woman with a history of hypertension, thyrotoxicosis, and poorly controlled diabetes on multiple oral hypoglycaemic agents presented with gradual onset progressive excessive hair growth without any virilizing features. On examination, she did not have Cushingnoid features or clitoromegaly. Her hirsutism was quantified with Ferriman-Gallwey score which was 9. Her biochemical evaluation showed elevated testosterone levels with normal DHEAS, ODST, 17-OHP, and prolactin. Low-dose dexamethasone suppression test did not suppress testosterone more than 40%. Contrast-enhanced CT of the adrenal and pelvis did not show any adrenal or ovarian mass lesions. Transvaginal ultrasound scan showed bilateral prominent ovaries only. Combined adrenal and ovarian venous sampling was carried out to localize the source of excess androgen, but only the left adrenal vein was successfully cannulated which showed suppressed testosterone level compared to periphery. The patient underwent total abdominal hysterectomy and bilateral salphingo oophorectomy, and her testosterone level normalized postoperatively. Her glycaemic control improved. Histology showed evidence of bilateral diffuse ovarian Leydig cell hyperplasia.
Conclusion: Evaluation of postmenopausal hirsutism needs careful history and examination followed by biochemical evaluation and imaging. While adrenal and ovarian venous sampling can help to arrive at a diagnosis, it is a technically demanding procedure with low success rates even at centers of excellence. Therefore, in such situations, bilateral oophorectomy may be the best course of action which will give the histological confirmation of the diagnosis. Successful treatment of hyperandrogenism can result in improvement of glycaemic control. Bilateral diffuse Leydig cell hyperplasia is a rare but important cause of postmenopausal hirsutism.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


