Orlaith C Brennan, John E Moore, Beverley C Millar
{"title":"Does social deprivation correlate with meningococcal MenACWY, Hib/MenC and 4CMenB/Meningococcal Group B vaccine uptake in Northern Ireland?","authors":"Orlaith C Brennan, John E Moore, Beverley C Millar","doi":"","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Several meningococcal vaccines have been recently introduced into the infant and adolescent vaccination schedules in Northern Ireland to promote immunity to <i>Neisseria meningitidis,</i> protecting against meningococcal septicaemia and meningococcal meningitis. Maintained vaccination uptake is vital in securing individual protection as well as herd immunity. Several social factors have been described in influencing vaccine uptake and therefore it was the aim of this study to examine possible correlations between meningococcal vaccine uptake rates and indicators of social deprivation in Northern Ireland.</p><p><strong>Methods: </strong>Vaccination data was retrieved from the Cover of Vaccination Evaluated Rapidly (COVER) database, for meningococcal vaccines (MenACWY, HiB/MenC & 4CMenB, as well as for MMR vaccine as a non-meningococcal control). Vaccine coverage data assessed included (i). Two doses of MenB by 12 months, (ii). All 3 doses of MenB by 24 months, (iii). HiB/MenC coverage, (iv). MenACWY (Year 12s, for NI) (v). First dose of MMR. Northern Ireland Multiple Deprivation Measures 2017 (NIMDM2017) were examined against 38 indicators in 7 domains. NI HSCT vaccine uptake dataset for each vaccine was correlated with each indicator in the HSCT NIMDM2017 dataset. Regression analysis was performed to determine the relationship between vaccine uptake and deprivation indicators and coefficient of variation (R<sup>2</sup>) was calculated for each of the indicators. R<sup>2</sup> values >0.7 were considered significant.</p><p><strong>Results: </strong>For 4CMenB (all 3 doses by 24 Months), HiB/MenC, MenACWY and for MMR, correlation of variation (R<sup>2</sup>) values > 0.7, were obtained for 17, 16, 0 and 17 social deprivation indicators, respectively. Significant deprivation indicators were (i) the proportion of 18-21 year olds, who have not enrolled in higher education courses at higher or further education establishments, (ii) the proportion of domestic dwellings that are unfit, (iii) the proportion of domestic dwellings with Local Area Problem Scores, (iv) rate of burglary, (v) rate of vehicle crime, (vi) rate of antisocial behaviour incidents (per 1,000 population), (vii) absenteeism at primary schools and (viii) the proportion of the population aged 65 and over living in households whose equivalised income is below 60% of the NI median.</p><p><strong>Conclusions: </strong>Within the last two decades, incidence of meningococcal disease has been on the decline. The introduction of meningococcal vaccines has contributed to this decrease and uptake of such vaccines should remain a public health priority to maintain the decline in meningococcal disease. Identifying contributing factors to low vaccine uptake, such as, the association between local deprivation and uptake of meningococcal vaccines, should be of public health importance and acknowledged by local governments and policy makers in their efforts to enhance vaccine uptake, both infant and teenage vaccination. There is a clear correlation with educational deprivation measures such as absenteeism and poor educational attainment and reduced vaccine uptake, perhaps through lack of understanding and willingness to vaccinate. This is where the importance of a clear and coherent public health message surrounding meningococcal vaccination should be prioritised, particularly to establish innovative modalities in a multidisciplinary team approach, to reach out to and increase vaccine uptake rates in socially deprived communities in Northern Ireland.</p>","PeriodicalId":38815,"journal":{"name":"Ulster Medical Journal","volume":"91 1","pages":"9-18"},"PeriodicalIF":0.0000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/09/f8/umj-91-01-9.PMC8835423.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Ulster Medical Journal","FirstCategoryId":"1085","ListUrlMain":"","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/2/11 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Several meningococcal vaccines have been recently introduced into the infant and adolescent vaccination schedules in Northern Ireland to promote immunity to Neisseria meningitidis, protecting against meningococcal septicaemia and meningococcal meningitis. Maintained vaccination uptake is vital in securing individual protection as well as herd immunity. Several social factors have been described in influencing vaccine uptake and therefore it was the aim of this study to examine possible correlations between meningococcal vaccine uptake rates and indicators of social deprivation in Northern Ireland.
Methods: Vaccination data was retrieved from the Cover of Vaccination Evaluated Rapidly (COVER) database, for meningococcal vaccines (MenACWY, HiB/MenC & 4CMenB, as well as for MMR vaccine as a non-meningococcal control). Vaccine coverage data assessed included (i). Two doses of MenB by 12 months, (ii). All 3 doses of MenB by 24 months, (iii). HiB/MenC coverage, (iv). MenACWY (Year 12s, for NI) (v). First dose of MMR. Northern Ireland Multiple Deprivation Measures 2017 (NIMDM2017) were examined against 38 indicators in 7 domains. NI HSCT vaccine uptake dataset for each vaccine was correlated with each indicator in the HSCT NIMDM2017 dataset. Regression analysis was performed to determine the relationship between vaccine uptake and deprivation indicators and coefficient of variation (R2) was calculated for each of the indicators. R2 values >0.7 were considered significant.
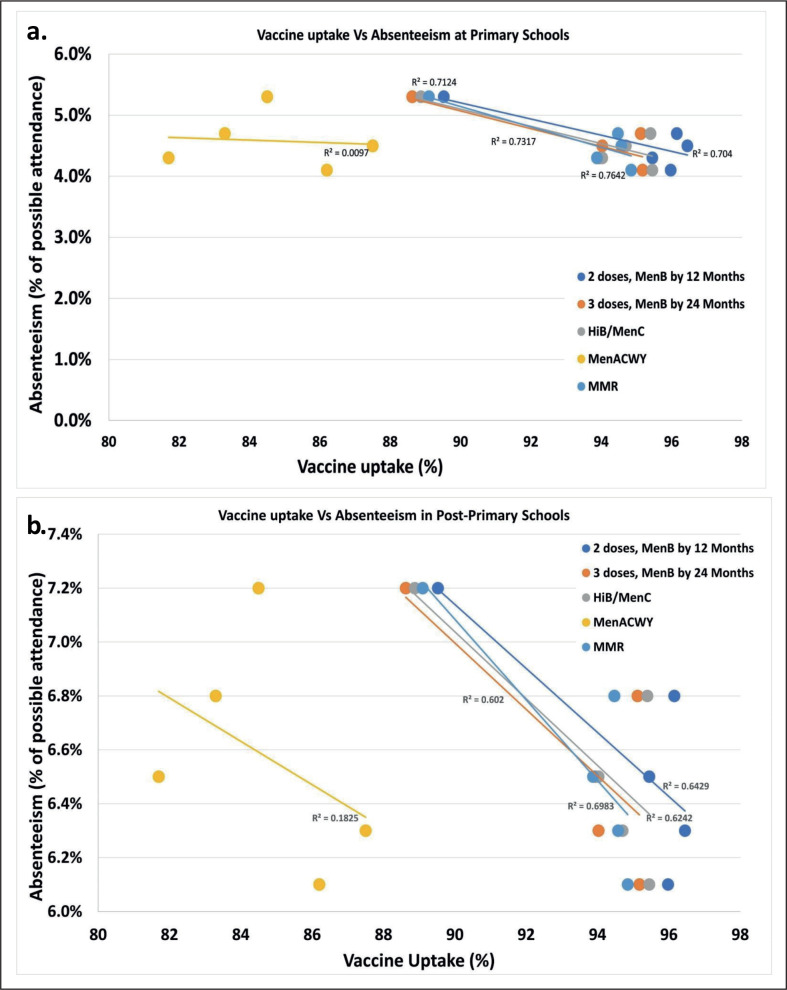
Results: For 4CMenB (all 3 doses by 24 Months), HiB/MenC, MenACWY and for MMR, correlation of variation (R2) values > 0.7, were obtained for 17, 16, 0 and 17 social deprivation indicators, respectively. Significant deprivation indicators were (i) the proportion of 18-21 year olds, who have not enrolled in higher education courses at higher or further education establishments, (ii) the proportion of domestic dwellings that are unfit, (iii) the proportion of domestic dwellings with Local Area Problem Scores, (iv) rate of burglary, (v) rate of vehicle crime, (vi) rate of antisocial behaviour incidents (per 1,000 population), (vii) absenteeism at primary schools and (viii) the proportion of the population aged 65 and over living in households whose equivalised income is below 60% of the NI median.
Conclusions: Within the last two decades, incidence of meningococcal disease has been on the decline. The introduction of meningococcal vaccines has contributed to this decrease and uptake of such vaccines should remain a public health priority to maintain the decline in meningococcal disease. Identifying contributing factors to low vaccine uptake, such as, the association between local deprivation and uptake of meningococcal vaccines, should be of public health importance and acknowledged by local governments and policy makers in their efforts to enhance vaccine uptake, both infant and teenage vaccination. There is a clear correlation with educational deprivation measures such as absenteeism and poor educational attainment and reduced vaccine uptake, perhaps through lack of understanding and willingness to vaccinate. This is where the importance of a clear and coherent public health message surrounding meningococcal vaccination should be prioritised, particularly to establish innovative modalities in a multidisciplinary team approach, to reach out to and increase vaccine uptake rates in socially deprived communities in Northern Ireland.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


