{"title":"Which injured patients with moderate fibrinogen deficit need fibrinogen supplementation?","authors":"Jean-Stephane David, Aline Lambert, Xavier-Jean Taverna, Pascal Incagnoli, Marie-Odile Geay-Baillat, Olivia Vassal, Arnaud Friggeri, Kenji Inaba","doi":"10.1186/s13049-021-00988-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In severely injured patients, fibrinogen supplementation is recommended when fibrinogenemia is < 1.5 g L<sup>-1</sup>, but some teams have suggested to use higher thresholds (fibrinogenemia < 2.0 g L<sup>-1</sup> or FIBTEM clot amplitude at 5 min (A5) values < 11 mm). The goal of this study was to specify in patients with a moderate fibrinogen deficit (MFD) whether some admission characteristics would be associated with fibrinogen administration at 24 h.</p><p><strong>Methods: </strong>Prospective analysis of retrospectively collected data from a trauma registry (01/2011-12/2019). MFD-C was defined by a fibrinogenemia 1.51-1.99 g L<sup>-1</sup> or the corresponding FIBTEM-A5 values (MFD-A5) that were determined from linear regression and ROC curve analysis. Administration of fibrinogen were described according to the following admission parameters: shock index (SI) > 1, hemoglobin level < 110 g L<sup>-1</sup> (HemoCue®), and base deficit > 5 mEq L<sup>-1</sup>. Data are expressed as count (%), median [IQR].</p><p><strong>Results: </strong>1076 patients were included in the study and 266 (27%) had MFD-C, among them, 122/266 (46%) received fibrinogen. Patients with MFD-C who received fibrinogen were more severely injured (ISS: 27 [19-36] vs. 24 [17-29]) and had more impaired vital signs (base deficit: 5.4 [3.6-7.8] vs. 3.8 [2.0-6.0]). Linear regression analysis found a positive correlation between fibrinogen level and FIBTEM-A5 (r: 0.805). For a fibrinogen level < 1.5 g L<sup>-1</sup> and < 2.0 g L<sup>-1</sup>, FIBTEM-A5 thresholds were 6 mm (sensitivity 85%, specificity 83%, AUC: 0.934) and 9 mm (sensitivity 84%, specificity 69%, AUC: 0.874), respectively. MFD-A5 values (185 (27%) patients) were defined as a FIBTEM-A5 between 7 and 9 mm. More than 50% of MFD-C patients presenting a SI > 1, a hemoglobin level < 110 g L<sup>-1</sup>, or a base deficit > 5.0 mEq L<sup>-1</sup> received fibrinogen. The relative risk [95% CI] for fibrinogen administration (SI > 1) were 1.39 [1.06-1.82] for MFD-C, and 2.17 [1.48-3.19] for MFD-A5. Results were not modified after adjustment on the ISS.</p><p><strong>Conclusions: </strong>We have shown in this study an association between shock parameters and fibrinogen administration. Further studies are needed to determine how these parameters may be used to guide fibrinogen administration in trauma patients with MFD.</p>","PeriodicalId":501057,"journal":{"name":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","volume":" ","pages":"174"},"PeriodicalIF":0.0000,"publicationDate":"2021-12-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8709958/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-021-00988-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: In severely injured patients, fibrinogen supplementation is recommended when fibrinogenemia is < 1.5 g L-1, but some teams have suggested to use higher thresholds (fibrinogenemia < 2.0 g L-1 or FIBTEM clot amplitude at 5 min (A5) values < 11 mm). The goal of this study was to specify in patients with a moderate fibrinogen deficit (MFD) whether some admission characteristics would be associated with fibrinogen administration at 24 h.
Methods: Prospective analysis of retrospectively collected data from a trauma registry (01/2011-12/2019). MFD-C was defined by a fibrinogenemia 1.51-1.99 g L-1 or the corresponding FIBTEM-A5 values (MFD-A5) that were determined from linear regression and ROC curve analysis. Administration of fibrinogen were described according to the following admission parameters: shock index (SI) > 1, hemoglobin level < 110 g L-1 (HemoCue®), and base deficit > 5 mEq L-1. Data are expressed as count (%), median [IQR].
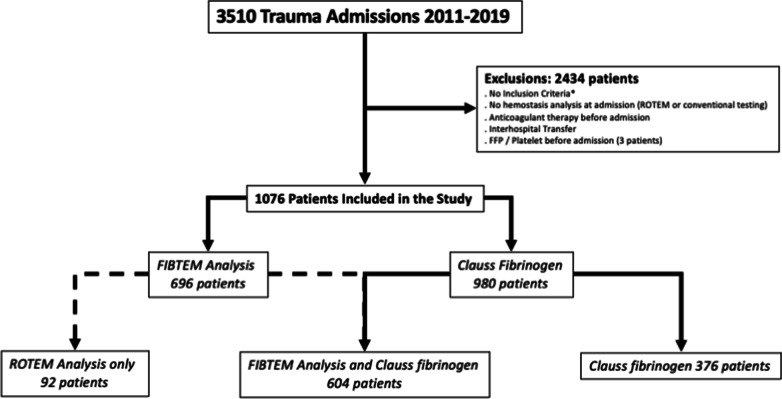
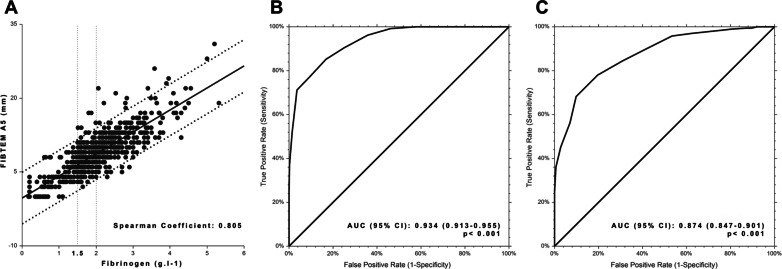
Results: 1076 patients were included in the study and 266 (27%) had MFD-C, among them, 122/266 (46%) received fibrinogen. Patients with MFD-C who received fibrinogen were more severely injured (ISS: 27 [19-36] vs. 24 [17-29]) and had more impaired vital signs (base deficit: 5.4 [3.6-7.8] vs. 3.8 [2.0-6.0]). Linear regression analysis found a positive correlation between fibrinogen level and FIBTEM-A5 (r: 0.805). For a fibrinogen level < 1.5 g L-1 and < 2.0 g L-1, FIBTEM-A5 thresholds were 6 mm (sensitivity 85%, specificity 83%, AUC: 0.934) and 9 mm (sensitivity 84%, specificity 69%, AUC: 0.874), respectively. MFD-A5 values (185 (27%) patients) were defined as a FIBTEM-A5 between 7 and 9 mm. More than 50% of MFD-C patients presenting a SI > 1, a hemoglobin level < 110 g L-1, or a base deficit > 5.0 mEq L-1 received fibrinogen. The relative risk [95% CI] for fibrinogen administration (SI > 1) were 1.39 [1.06-1.82] for MFD-C, and 2.17 [1.48-3.19] for MFD-A5. Results were not modified after adjustment on the ISS.
Conclusions: We have shown in this study an association between shock parameters and fibrinogen administration. Further studies are needed to determine how these parameters may be used to guide fibrinogen administration in trauma patients with MFD.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


