Martin Lindgren, Susanne J Nielsen, Erik Björklund, Aldina Pivodic, Sossio Perrotta, Emma C Hansson, Anders Jeppsson, Andreas Martinsson
{"title":"Beta blockers and long-term outcome after coronary artery bypass grafting: a nationwide observational study.","authors":"Martin Lindgren, Susanne J Nielsen, Erik Björklund, Aldina Pivodic, Sossio Perrotta, Emma C Hansson, Anders Jeppsson, Andreas Martinsson","doi":"10.1093/ehjcvp/pvac006","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Beta blockers are associated with improved outcomes for selected patients with cardiovascular disease. We assessed long-term utilization of beta blockers after coronary artery bypass grafting (CABG) and its association with outcome.</p><p><strong>Methods and results: </strong>All 35 184 patients in Sweden who underwent first-time isolated CABG between 1 January 2006 and 31 December 2017 and were followed for at least 6 months were included in a nationwide observational study. Multivariable Cox regression models using time-updated data on dispensed prescriptions were used to assess associations between different types of beta blockers and outcomes. The primary outcome was major adverse cardiovascular events (MACEs), a composite of all-cause mortality, stroke, and myocardial infarction (MI). Subgroup analyses were performed in patients with and without previous MI, heart failure, and reduced left ventricular ejection fraction (LVEF). Median follow-up was 5.2 years (range 0-11). At baseline, 33 159 (94.2%) patients were dispensed beta blockers, 30 563 (92.2%) of which were cardioselective beta blockers. After 10 years, the dispensing of cardioselective beta blockers had declined to 73.7% of all patients. Ongoing treatment with cardioselective beta blockers was associated with a slight reduction in MACEs [hazard ratio (HR) 0.93, 95% confidence interval (CI) 0.89-0.98, P = 0.0063]. The reduction was largely driven by a reduced risk of MI (HR 0.83, 95% CI 0.75-0.92, P = 0.0003), while there was no significant reduction in all-cause mortality (HR 0.99, 95% CI 0.93-1.05) and stroke (HR 0.96, 95% CI 0.87-1.05). The reduced risk for MI was consistent in all the investigated subgroups.</p><p><strong>Conclusion: </strong>Ongoing treatment with cardioselective beta blockers after CABG is associated with a reduction in MACEs, mainly because of reduced long-term risk for MI. The association between cardioselective beta blockers and MI was consistent in patients with and patients without previous MI, heart failure, atrial fibrillation, or reduced LVEF.</p>","PeriodicalId":11995,"journal":{"name":"European Heart Journal — Cardiovascular Pharmacotherapy","volume":" ","pages":"529-536"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/52/24/pvac006.PMC9366641.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal — Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvac006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Aims: Beta blockers are associated with improved outcomes for selected patients with cardiovascular disease. We assessed long-term utilization of beta blockers after coronary artery bypass grafting (CABG) and its association with outcome.
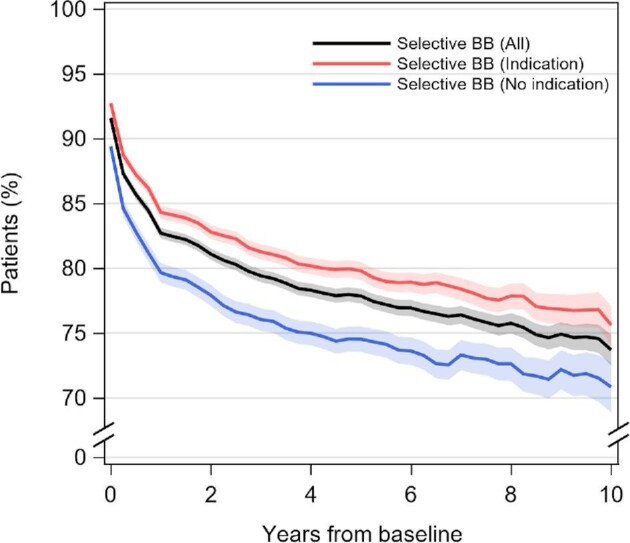
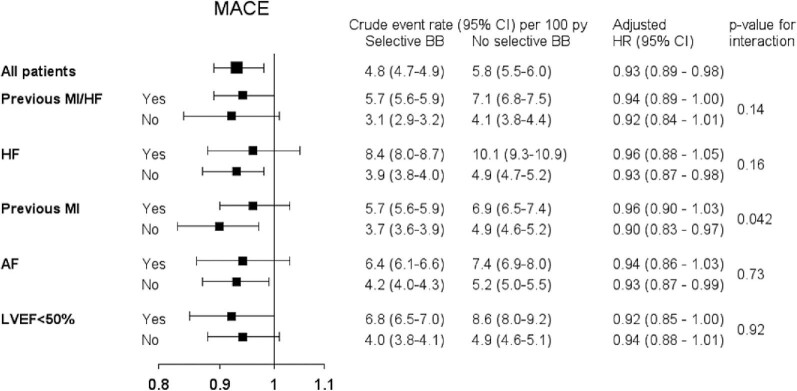
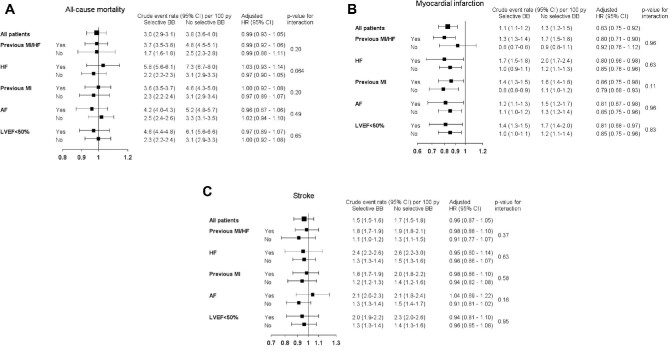
Methods and results: All 35 184 patients in Sweden who underwent first-time isolated CABG between 1 January 2006 and 31 December 2017 and were followed for at least 6 months were included in a nationwide observational study. Multivariable Cox regression models using time-updated data on dispensed prescriptions were used to assess associations between different types of beta blockers and outcomes. The primary outcome was major adverse cardiovascular events (MACEs), a composite of all-cause mortality, stroke, and myocardial infarction (MI). Subgroup analyses were performed in patients with and without previous MI, heart failure, and reduced left ventricular ejection fraction (LVEF). Median follow-up was 5.2 years (range 0-11). At baseline, 33 159 (94.2%) patients were dispensed beta blockers, 30 563 (92.2%) of which were cardioselective beta blockers. After 10 years, the dispensing of cardioselective beta blockers had declined to 73.7% of all patients. Ongoing treatment with cardioselective beta blockers was associated with a slight reduction in MACEs [hazard ratio (HR) 0.93, 95% confidence interval (CI) 0.89-0.98, P = 0.0063]. The reduction was largely driven by a reduced risk of MI (HR 0.83, 95% CI 0.75-0.92, P = 0.0003), while there was no significant reduction in all-cause mortality (HR 0.99, 95% CI 0.93-1.05) and stroke (HR 0.96, 95% CI 0.87-1.05). The reduced risk for MI was consistent in all the investigated subgroups.
Conclusion: Ongoing treatment with cardioselective beta blockers after CABG is associated with a reduction in MACEs, mainly because of reduced long-term risk for MI. The association between cardioselective beta blockers and MI was consistent in patients with and patients without previous MI, heart failure, atrial fibrillation, or reduced LVEF.
目的:β受体阻滞剂与特定心血管疾病患者预后改善相关。我们评估了冠状动脉旁路移植术(CABG)后β受体阻滞剂的长期使用及其与预后的关系。方法和结果:2006年1月1日至2017年12月31日期间,瑞典所有35184例首次行置换性冠脉搭桥的患者被纳入一项全国性观察性研究,随访时间至少为6个月。多变量Cox回归模型使用时间更新的处方数据来评估不同类型的受体阻滞剂与结果之间的关联。主要终点是主要不良心血管事件(mace),由全因死亡率、卒中和心肌梗死(MI)组成。亚组分析在有或没有心肌梗死、心力衰竭和左心室射血分数(LVEF)降低的患者中进行。中位随访时间为5.2年(0-11年)。基线时,33 159例(94.2%)患者使用β受体阻滞剂,其中30 563例(92.2%)为心脏选择性β受体阻滞剂。10年后,心脏选择性受体阻滞剂的配药率下降到73.7%。持续使用心脏选择性受体阻滞剂治疗与mace的轻微降低相关[风险比(HR) 0.93, 95%可信区间(CI) 0.89-0.98, P = 0.0063]。降低的主要原因是心肌梗死风险降低(HR 0.83, 95% CI 0.75-0.92, P = 0.0003),而全因死亡率(HR 0.99, 95% CI 0.93-1.05)和中风(HR 0.96, 95% CI 0.87-1.05)没有显著降低。在所有被调查的亚组中,心肌梗死风险的降低是一致的。结论:CABG后持续使用心脏选择性β受体阻滞剂治疗与心肌梗死发生率降低相关,主要是因为心肌梗死的长期风险降低。心脏选择性β受体阻滞剂与心肌梗死之间的相关性在有和没有心肌梗死、心力衰竭、心房颤动或LVEF降低的患者中是一致的。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


