Navindra Persaud, Kevin E Thorpe, Michael Bedard, Stephen W Hwang, Andrew Pinto, Peter Jüni, Bruno R da Costa
{"title":"Cash transfer during the COVID-19 pandemic: a multicentre, randomised controlled trial.","authors":"Navindra Persaud, Kevin E Thorpe, Michael Bedard, Stephen W Hwang, Andrew Pinto, Peter Jüni, Bruno R da Costa","doi":"10.1136/fmch-2021-001452","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To evaluate the effect of a one-time cash transfer of $C1000 in people who are unable to physically distance due to insufficient income.</p><p><strong>Design: </strong>Open-label, multi-centre, randomised superiority trial.</p><p><strong>Setting: </strong>Seven primary care sites in Ontario, Canada; six urban sites associated with St. Michael's Hospital in Toronto and one in Manitoulin Island.</p><p><strong>Participants: </strong>392 individuals who reported trouble affording basic necessities due to disruptions related to COVID-19.</p><p><strong>Intervention: </strong>After random allocation, participants either received the cash transfer of $C1000 (n=196) or physical distancing guidelines alone (n=196).</p><p><strong>Main outcome measures: </strong>The primary outcome was the maximum number of symptoms consistent with COVID-19 over 14 days. Secondary outcomes were meeting clinical criteria for COVID-19, SARS-CoV-2 presence, number of close contacts, general health and ability to afford basic necessities.</p><p><strong>Results: </strong>The primary outcome of number of symptoms reported by participants did not differ between groups after 2 weeks (cash transfer, mean 1.6 vs 1.9, ratio of means 0.83; 95% CI 0.56 to 1.24). There were no statistically significant effects on secondary outcomes of the meeting COVID-19 clinical criteria (7.9% vs 12.8%; risk difference -0.05; 95% CI -0.11 to 0.01), SARS-CoV-2 presence (0.5% vs 0.6%; risk difference 0.00 95% CI -0.02 to 0.02), mean number of close contacts (3.5 vs 3.7; rate ratio 1.10; 95% CI 0.83 to 1.46), general health very good or excellent (60% vs 63%; risk difference -0.03 95% CI -0.14 to 0.08) and ability to make ends meet (52% vs 51%; risk difference 0.01 95% CI -0.10 to 0.12).</p><p><strong>Conclusions: </strong>A single cash transfer did not reduce the COVID-19 symptoms or improve the ability to afford necessities. Further studies are needed to determine whether some groups may benefit from financial supports and to determine if a higher level of support is beneficial.</p><p><strong>Trial registration number: </strong>NCT04359264.</p>","PeriodicalId":44590,"journal":{"name":"Family Medicine and Community Health","volume":"9 4","pages":""},"PeriodicalIF":2.6000,"publicationDate":"2021-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8b/61/fmch-2021-001452.PMC8662581.pdf","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Family Medicine and Community Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/fmch-2021-001452","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PRIMARY HEALTH CARE","Score":null,"Total":0}
引用次数: 6
Abstract
Objective: To evaluate the effect of a one-time cash transfer of $C1000 in people who are unable to physically distance due to insufficient income.
Setting: Seven primary care sites in Ontario, Canada; six urban sites associated with St. Michael's Hospital in Toronto and one in Manitoulin Island.
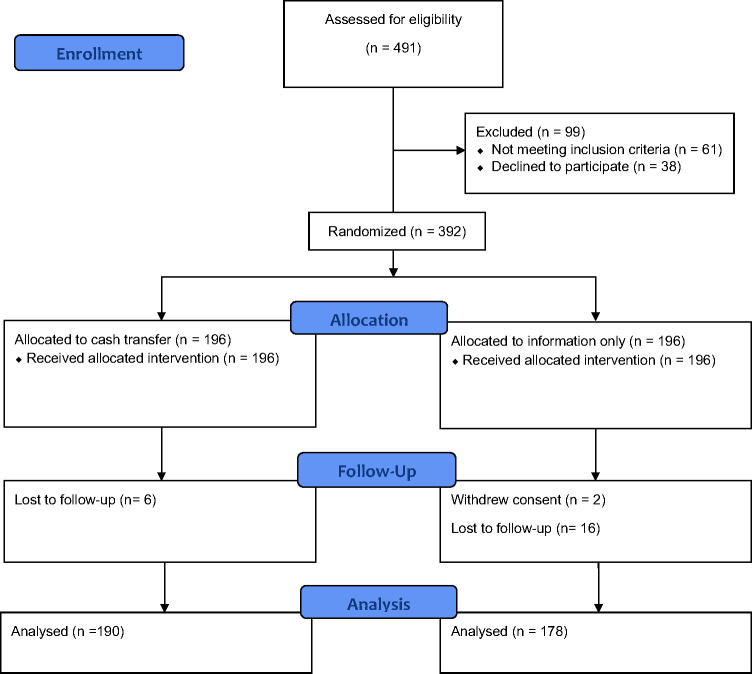
Participants: 392 individuals who reported trouble affording basic necessities due to disruptions related to COVID-19.
Intervention: After random allocation, participants either received the cash transfer of $C1000 (n=196) or physical distancing guidelines alone (n=196).
Main outcome measures: The primary outcome was the maximum number of symptoms consistent with COVID-19 over 14 days. Secondary outcomes were meeting clinical criteria for COVID-19, SARS-CoV-2 presence, number of close contacts, general health and ability to afford basic necessities.
Results: The primary outcome of number of symptoms reported by participants did not differ between groups after 2 weeks (cash transfer, mean 1.6 vs 1.9, ratio of means 0.83; 95% CI 0.56 to 1.24). There were no statistically significant effects on secondary outcomes of the meeting COVID-19 clinical criteria (7.9% vs 12.8%; risk difference -0.05; 95% CI -0.11 to 0.01), SARS-CoV-2 presence (0.5% vs 0.6%; risk difference 0.00 95% CI -0.02 to 0.02), mean number of close contacts (3.5 vs 3.7; rate ratio 1.10; 95% CI 0.83 to 1.46), general health very good or excellent (60% vs 63%; risk difference -0.03 95% CI -0.14 to 0.08) and ability to make ends meet (52% vs 51%; risk difference 0.01 95% CI -0.10 to 0.12).
Conclusions: A single cash transfer did not reduce the COVID-19 symptoms or improve the ability to afford necessities. Further studies are needed to determine whether some groups may benefit from financial supports and to determine if a higher level of support is beneficial.
目的:评估一次性现金转移1000加元对因收入不足而无法进行身体距离的人的影响。设计:开放标签、多中心、随机优势试验。环境:加拿大安大略省的七个初级保健站点;六个与多伦多圣迈克尔医院有关的城市地点和一个在马尼图林岛。参与者:392名报告因COVID-19相关中断而无法负担基本必需品的个人。干预:随机分配后,参与者要么获得1000加元的现金转移(n=196),要么单独获得物理距离指南(n=196)。主要结局指标:主要结局指标为14天内符合COVID-19症状的最大次数。次要指标为符合COVID-19临床标准、是否存在SARS-CoV-2、密切接触者人数、总体健康状况和负担基本必需品的能力。结果:2周后,两组受试者报告的主要结局症状数无差异(现金转移,平均1.6 vs 1.9,平均比值0.83;95% CI 0.56 ~ 1.24)。符合COVID-19临床标准的次要结局无统计学意义(7.9% vs 12.8%;风险差异-0.05;95% CI -0.11至0.01),SARS-CoV-2存在(0.5%对0.6%;风险差0.00 95% CI -0.02 ~ 0.02),平均密切接触者人数(3.5 vs 3.7;比率1.10;95% CI 0.83 - 1.46),总体健康状况非常好或极好(60% vs 63%;风险差异-0.03 95% CI -0.14至0.08)和维持收支平衡的能力(52%对51%;风险差0.01 (95% CI -0.10 ~ 0.12)。结论:单次现金转移并不能减轻COVID-19症状或提高支付必需品的能力。需要进行进一步的研究,以确定某些群体是否可以从财政支助中受益,并确定更高水平的支助是否有益。试验注册号:NCT04359264。
期刊介绍:
Family Medicine and Community Health (FMCH) is a peer-reviewed, open-access journal focusing on the topics of family medicine, general practice and community health. FMCH strives to be a leading international journal that promotes ‘Health Care for All’ through disseminating novel knowledge and best practices in primary care, family medicine, and community health. FMCH publishes original research, review, methodology, commentary, reflection, and case-study from the lens of population health. FMCH’s Asian Focus section features reports of family medicine development in the Asia-pacific region. FMCH aims to be an exemplary forum for the timely communication of medical knowledge and skills with the goal of promoting improved health care through the practice of family and community-based medicine globally. FMCH aims to serve a diverse audience including researchers, educators, policymakers and leaders of family medicine and community health. We also aim to provide content relevant for researchers working on population health, epidemiology, public policy, disease control and management, preventative medicine and disease burden. FMCH does not impose any article processing charges (APC) or submission charges.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


