{"title":"Hematinic and Iron Optimization in Peri-operative Anemia and Iron Deficiency.","authors":"Lachlan F Miles, Toby Richards","doi":"10.1007/s40140-021-00503-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose of review: </strong>Preoperative anemia is independently associated with worse postoperative outcomes following cardiac and noncardiac surgery. This article explores the current understanding of perioperative anemia and iron deficiency with reference to definition, diagnosis, and treatment.</p><p><strong>Recent findings: </strong>Iron deficiency is the most common cause of anemia. It can arise from reduced iron intake, poor absorption, or excess iron loss. Inflammation throughout the preoperative period can drive iron sequestration, leading to a functional deficiency of iron and the development of what was referred to until recently as the \"anemia of chronic disease.\" Current best practice guidance supports the routine administration of preoperative intravenous iron to treat anemia despite limited evidence. This \"one size fits all\" approach has been called into question following results from a recent large, randomized trial (the PREVENTT trial) that assessed the use of a single dose of intravenous iron compared to placebo 10-42 days before major abdominal surgery. Although there were no improvements in patient-centered outcomes apparent during the initial hospital stay, secondary endpoints of this trial suggested there may be some late benefit after discharge from the hospital (8 weeks postoperatively). This trial raises questions on (1) the mechanisms of iron deficiency in the perioperative patient; (2) the need to reassess our opinions on generic anemia management; and (3) the need to address patient outcomes after discharge from hospital.</p><p><strong>Summary: </strong>Despite the known associations between preoperative anemia (particularly iron deficiency anemia) and poor postoperative outcome, recent evidence suggests that administering intravenous iron relatively close to surgery does not yield a tangible short-term benefit. This is made more complex by the interplay between iron and innate immunity. Iron deficiency irrespective of hemoglobin concentration may also impact postoperative outcomes. Therefore, further research into associations between iron deficiency and postoperative outcomes, and between postoperative anemia, delayed outcomes (hospital readmission), and the efficacy of postoperative intravenous iron is required.</p>","PeriodicalId":36608,"journal":{"name":"Current Anesthesiology Reports","volume":"12 1","pages":"65-77"},"PeriodicalIF":1.6000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8766356/pdf/","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Current Anesthesiology Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40140-021-00503-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/19 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 3
Abstract
Purpose of review: Preoperative anemia is independently associated with worse postoperative outcomes following cardiac and noncardiac surgery. This article explores the current understanding of perioperative anemia and iron deficiency with reference to definition, diagnosis, and treatment.
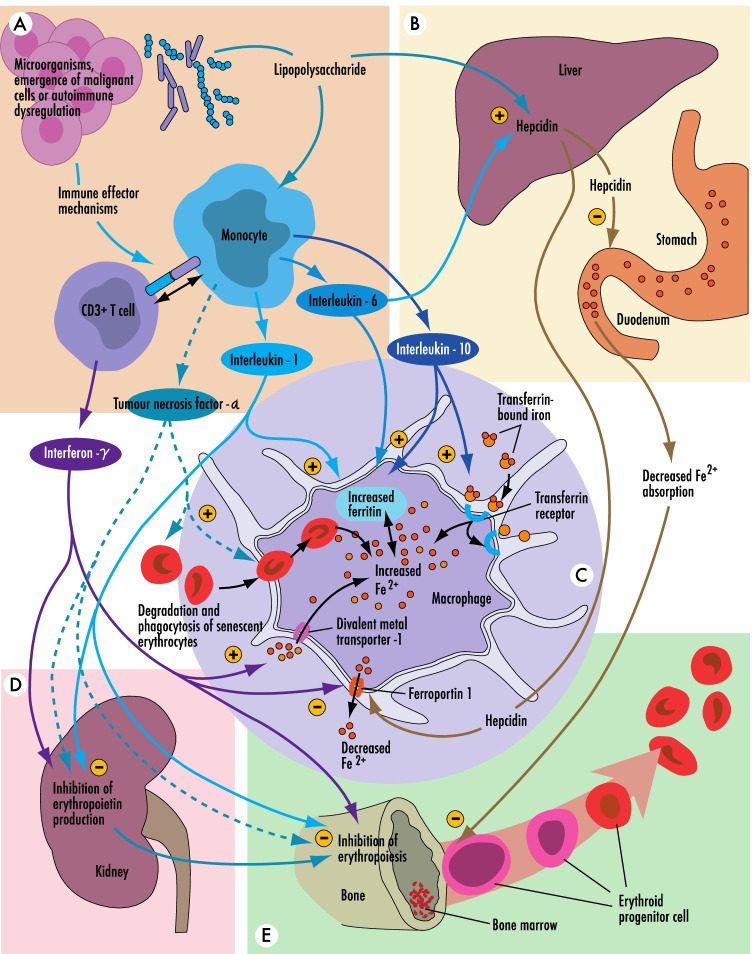
Recent findings: Iron deficiency is the most common cause of anemia. It can arise from reduced iron intake, poor absorption, or excess iron loss. Inflammation throughout the preoperative period can drive iron sequestration, leading to a functional deficiency of iron and the development of what was referred to until recently as the "anemia of chronic disease." Current best practice guidance supports the routine administration of preoperative intravenous iron to treat anemia despite limited evidence. This "one size fits all" approach has been called into question following results from a recent large, randomized trial (the PREVENTT trial) that assessed the use of a single dose of intravenous iron compared to placebo 10-42 days before major abdominal surgery. Although there were no improvements in patient-centered outcomes apparent during the initial hospital stay, secondary endpoints of this trial suggested there may be some late benefit after discharge from the hospital (8 weeks postoperatively). This trial raises questions on (1) the mechanisms of iron deficiency in the perioperative patient; (2) the need to reassess our opinions on generic anemia management; and (3) the need to address patient outcomes after discharge from hospital.
Summary: Despite the known associations between preoperative anemia (particularly iron deficiency anemia) and poor postoperative outcome, recent evidence suggests that administering intravenous iron relatively close to surgery does not yield a tangible short-term benefit. This is made more complex by the interplay between iron and innate immunity. Iron deficiency irrespective of hemoglobin concentration may also impact postoperative outcomes. Therefore, further research into associations between iron deficiency and postoperative outcomes, and between postoperative anemia, delayed outcomes (hospital readmission), and the efficacy of postoperative intravenous iron is required.
期刊介绍:
This journal aims to offer expert review articles on the most significant recent developments in the field of anesthesiology. By providing clear, insightful, balanced contributions, the journal intends to serve those involved in the delivery of anesthesia for surgical and medical procedures, treatment of acute and chronic pain conditions, perioperative management for operative and intensive care unit patients, and associated basic science and clinical research efforts in their areas. We accomplish this aim by appointing international authorities to serve as Section Editors in key subject areas across the field. Section Editors select topics for which leading experts contribute comprehensive review articles that emphasize new developments and recently published papers of major importance, highlighted by annotated reference lists. An Editorial Board of more than 20 internationally diverse members reviews the annual table of contents, ensures that topics include emerging research, and suggests topics of special importance to their country/region. Topics covered may include ambulatory anesthesia; anesthesia and inflammation; anesthetic mechanisms; anesthetic pharmacology; cardiovascular anesthesia; critical care anesthesia; local anesthetic pharmacology; monitoring technology; neuroanesthesia; neuromuscular blockade; obstetrical anesthesia; pain mechanisms; pain therapy; patient safety; pediatric anesthesia; quality assessment; regional anesthesia; and transplantation anesthesia.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


