IgG4-Mediated Neurologic Autoimmunities: Understanding the Pathogenicity of IgG4, Ineffectiveness of IVIg, and Long-Lasting Benefits of Anti-B Cell Therapies.
{"title":"IgG4-Mediated Neurologic Autoimmunities: Understanding the Pathogenicity of IgG4, Ineffectiveness of IVIg, and Long-Lasting Benefits of Anti-B Cell Therapies.","authors":"Marinos C Dalakas","doi":"10.1212/NXI.0000000000001116","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>Describe the unique functions of immunoglobulin G4 (IgG4) in IgG4-neurologic disorders (IgG4-ND) and explain why, in contrast to their IgG1-counterparts, they respond poorly to intravenous immune globulin (IVIg) but effectively to anti-B cell therapies.</p><p><strong>Methods: </strong>The IgG4 structure and isotype switch, B cells and plasmablasts relevant to IgG4 production, and IgG4-induced disruption of the targeted antigens are reviewed and compared with IgG1-mediated autoimmune ND, where IVIg inhibits IgG1-triggered inflammatory effects.</p><p><strong>Results: </strong>The main IgG4-ND include muscle-specific kinase myasthenia; nodal/paranodal chronic inflammatory demyelinating polyradiculoneuropathy with antibodies to neurofascin-155, contactin-1/caspr-1, or pan-neurofascins; antileucine-rich, glioma-inactivated-1 and contactin-associated protein-like 2 associated-limbic encephalitis, Morvan syndrome, or neuromyotonia; and anti-IgLON5 disorder. The IgG4, because of its unique structural features in the hinge region, has noninflammatory properties being functionally monovalent and bispecific, unable to engage in cross-linking and internalization of the targeted antigen. In contrast to IgG1 subclass which is bivalent and monospecific, IgG4 does not activate complement and cannot bind to inhibitory Fcγ receptor (FcγRIIb) to activate cellular and complement-mediated immune responses, the key functions inhibited by IVIg. Because IVIg contains only 0.7%-2.6% IgG4, its idiotypes are of IgG1 subclass and cannot effectively neutralize IgG4 or sufficiently enhance IgG4 catabolism by saturating FcRn. In contrast, rituximab, by targeting memory B cells and IgG4-producing CD20-positive short-lived plasma cells, induces long-lasting clinical benefits.</p><p><strong>Discussion: </strong>Rituximab is the preferred treatment in IgG4-ND patients with severe disease by effectively targeting the production of pathogenic IgG-4 antibodies. In contrast, IVIG is ineffective because it inhibits immunoinflammatory functions irrelevant to the mechanistic effects of IgG4 and contains IgG-1 idiotypes that cannot sufficiently neutralize or possibly catabolize IgG4. Controlled studies with anti-CD19/20 monoclonals that also activate FcγRIIb may be more promising in treating IgG4-ND.</p>","PeriodicalId":520720,"journal":{"name":"Neurology(R) neuroimmunology & neuroinflammation","volume":" ","pages":""},"PeriodicalIF":7.5000,"publicationDate":"2021-11-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/3a/52/NEURIMMINFL2021039399.PMC8630661.pdf","citationCount":"17","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurology(R) neuroimmunology & neuroinflammation","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1212/NXI.0000000000001116","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2022/1/1 0:00:00","PubModel":"Print","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 17
Abstract
Background and objectives: Describe the unique functions of immunoglobulin G4 (IgG4) in IgG4-neurologic disorders (IgG4-ND) and explain why, in contrast to their IgG1-counterparts, they respond poorly to intravenous immune globulin (IVIg) but effectively to anti-B cell therapies.
Methods: The IgG4 structure and isotype switch, B cells and plasmablasts relevant to IgG4 production, and IgG4-induced disruption of the targeted antigens are reviewed and compared with IgG1-mediated autoimmune ND, where IVIg inhibits IgG1-triggered inflammatory effects.
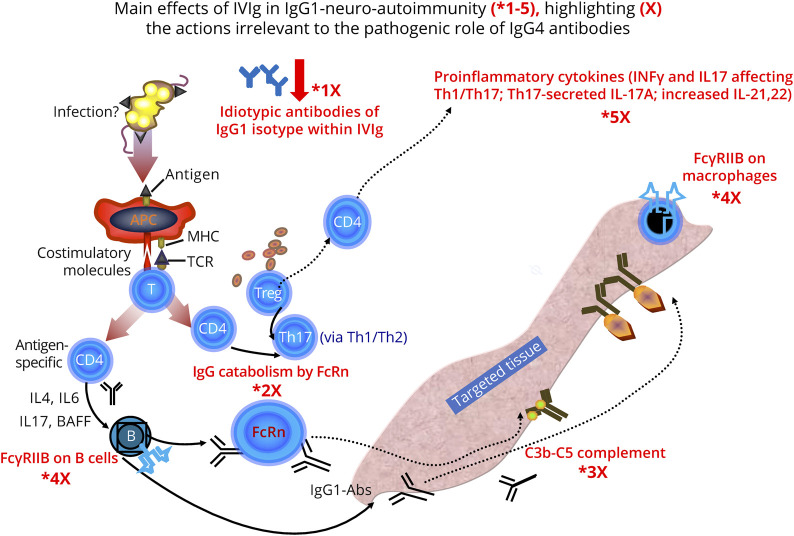
Results: The main IgG4-ND include muscle-specific kinase myasthenia; nodal/paranodal chronic inflammatory demyelinating polyradiculoneuropathy with antibodies to neurofascin-155, contactin-1/caspr-1, or pan-neurofascins; antileucine-rich, glioma-inactivated-1 and contactin-associated protein-like 2 associated-limbic encephalitis, Morvan syndrome, or neuromyotonia; and anti-IgLON5 disorder. The IgG4, because of its unique structural features in the hinge region, has noninflammatory properties being functionally monovalent and bispecific, unable to engage in cross-linking and internalization of the targeted antigen. In contrast to IgG1 subclass which is bivalent and monospecific, IgG4 does not activate complement and cannot bind to inhibitory Fcγ receptor (FcγRIIb) to activate cellular and complement-mediated immune responses, the key functions inhibited by IVIg. Because IVIg contains only 0.7%-2.6% IgG4, its idiotypes are of IgG1 subclass and cannot effectively neutralize IgG4 or sufficiently enhance IgG4 catabolism by saturating FcRn. In contrast, rituximab, by targeting memory B cells and IgG4-producing CD20-positive short-lived plasma cells, induces long-lasting clinical benefits.
Discussion: Rituximab is the preferred treatment in IgG4-ND patients with severe disease by effectively targeting the production of pathogenic IgG-4 antibodies. In contrast, IVIG is ineffective because it inhibits immunoinflammatory functions irrelevant to the mechanistic effects of IgG4 and contains IgG-1 idiotypes that cannot sufficiently neutralize or possibly catabolize IgG4. Controlled studies with anti-CD19/20 monoclonals that also activate FcγRIIb may be more promising in treating IgG4-ND.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


