Comparison of peak expiratory Flow(PEF) and COPD assessment test (CAT) to assess COPD exacerbation requiring hospitalization: A prospective observational study.
{"title":"Comparison of peak expiratory Flow(PEF) and COPD assessment test (CAT) to assess COPD exacerbation requiring hospitalization: A prospective observational study.","authors":"Jie Cen, Lei Weng","doi":"10.1177/14799731221081859","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Acute exacerbation of chronic obstructive pulmonary disease (COPD) resulting in hospitalization is significantly associated with the increased morbidity and mortality, but there is a lack of an effective method to assess it. This study aimed to compare the ability of peak expiratory flow (PEF) and COPD assessment test (CAT) to assess COPD exacerbations requiring hospitalization.</p><p><strong>Methods: </strong>A cohort of 110 patients with moderate to severe COPD was studied over a period of 12 months, and their daily morning PEFs and CAT scores were recorded throughout the study.</p><p><strong>Results: </strong>After 12 months of follow-up, 72 patients experienced 156 COPD exacerbations, 74 (47%) that resulted in hospitalization and 82 (53%) that did not result in hospitalization. Change in CAT score from baseline to exacerbation was significantly related to change in PEF and Spearman's rho =0.375 (95% CI, 0.227 to 0.506; p < .001). Change in PEF and CAT score from baseline to hospitalized exacerbation was significantly larger than that from baseline to non-hospitalized exacerbation (p < .05). Multivariable analysis indicated that ΔPEF (OR 1.11, 95% CI 1.06-1.16, p < .001) and ΔCAT (OR 1.64 95% CI 1.18-2.27, p = .003) were independently associated with risk of hospitalized exacerbation. ROC analysis indicated that the optimal cutoff value of ΔPEF for identifying hospitalized exacerbation was 49 L/min (27% from baseline), with a sensitivity and specificity of 82.7% and 76.7% (area under the curve [AUC] = 0.872 (95% CI 0.80-0.944, p < .05). The optimal cutoff value of ΔCAT score for identifying hospitalized exacerbation was 10.5 (63% from baseline), with a sensitivity and specificity of 67.3% and 77.4% [AUC]=0.763 (95% CI 0.67-0.857, p < .05). The AUC of ΔPEF and ΔCAT combined for the identification of hospitalized exacerbation was 0.900 (95% CI 0.841-0.959, p < .05), which was larger than that of ΔCAT or ΔPEF.</p><p><strong>Conclusions: </strong>ΔPEF and ΔCAT were independently associated with risk of hospitalized exacerbation. Compared with CAT, PEF was superior to identify hospitalized exacerbation. Identification via PEF and CAT combined is more effective than using PEF or CAT alone. These results help to assess the severity of COPD exacerbation and provide valuable information for clinical decision-making.</p>","PeriodicalId":10217,"journal":{"name":"Chronic Respiratory Disease","volume":" ","pages":"14799731221081859"},"PeriodicalIF":2.3000,"publicationDate":"2022-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/9e/89/10.1177_14799731221081859.PMC8883293.pdf","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Chronic Respiratory Disease","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/14799731221081859","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Acute exacerbation of chronic obstructive pulmonary disease (COPD) resulting in hospitalization is significantly associated with the increased morbidity and mortality, but there is a lack of an effective method to assess it. This study aimed to compare the ability of peak expiratory flow (PEF) and COPD assessment test (CAT) to assess COPD exacerbations requiring hospitalization.
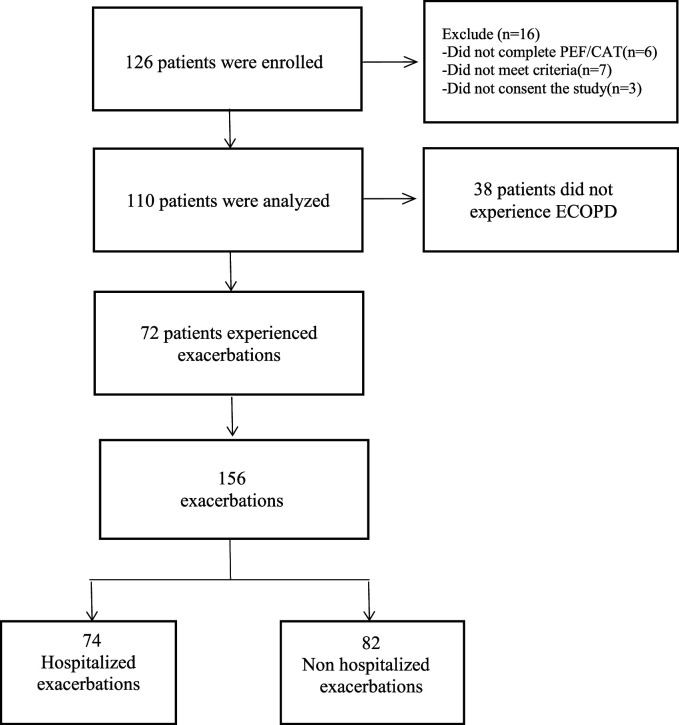
Methods: A cohort of 110 patients with moderate to severe COPD was studied over a period of 12 months, and their daily morning PEFs and CAT scores were recorded throughout the study.
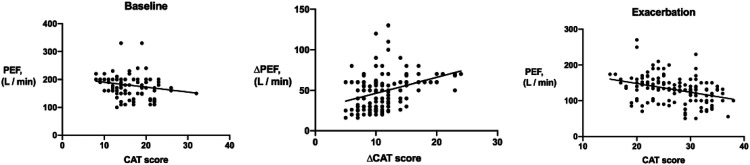
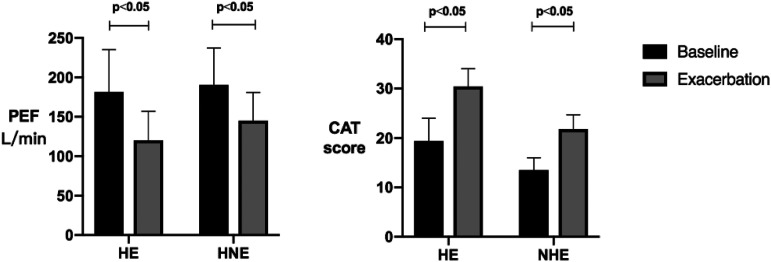
Results: After 12 months of follow-up, 72 patients experienced 156 COPD exacerbations, 74 (47%) that resulted in hospitalization and 82 (53%) that did not result in hospitalization. Change in CAT score from baseline to exacerbation was significantly related to change in PEF and Spearman's rho =0.375 (95% CI, 0.227 to 0.506; p < .001). Change in PEF and CAT score from baseline to hospitalized exacerbation was significantly larger than that from baseline to non-hospitalized exacerbation (p < .05). Multivariable analysis indicated that ΔPEF (OR 1.11, 95% CI 1.06-1.16, p < .001) and ΔCAT (OR 1.64 95% CI 1.18-2.27, p = .003) were independently associated with risk of hospitalized exacerbation. ROC analysis indicated that the optimal cutoff value of ΔPEF for identifying hospitalized exacerbation was 49 L/min (27% from baseline), with a sensitivity and specificity of 82.7% and 76.7% (area under the curve [AUC] = 0.872 (95% CI 0.80-0.944, p < .05). The optimal cutoff value of ΔCAT score for identifying hospitalized exacerbation was 10.5 (63% from baseline), with a sensitivity and specificity of 67.3% and 77.4% [AUC]=0.763 (95% CI 0.67-0.857, p < .05). The AUC of ΔPEF and ΔCAT combined for the identification of hospitalized exacerbation was 0.900 (95% CI 0.841-0.959, p < .05), which was larger than that of ΔCAT or ΔPEF.
Conclusions: ΔPEF and ΔCAT were independently associated with risk of hospitalized exacerbation. Compared with CAT, PEF was superior to identify hospitalized exacerbation. Identification via PEF and CAT combined is more effective than using PEF or CAT alone. These results help to assess the severity of COPD exacerbation and provide valuable information for clinical decision-making.
背景:慢性阻塞性肺疾病(COPD)急性加重导致住院与发病率和死亡率增加显著相关,但缺乏有效的评估方法。本研究旨在比较呼气峰流量(PEF)和COPD评估试验(CAT)评估COPD急性加重需要住院治疗的能力。方法:对110例中重度COPD患者进行了为期12个月的研究,并在整个研究过程中记录了他们每天早晨的pef和CAT评分。结果:经过12个月的随访,72例患者经历了156次COPD加重,74例(47%)导致住院,82例(53%)未导致住院。CAT评分从基线到加重期的变化与PEF和Spearman的变化显著相关(95% CI, 0.227 ~ 0.506;P < 0.001)。PEF和CAT评分从基线到住院加重的变化明显大于基线到非住院加重的变化(p < 0.05)。多变量分析显示ΔPEF (OR 1.11, 95% CI 1.06-1.16, p < .001)和ΔCAT (OR 1.64 95% CI 1.18-2.27, p = .003)与住院加重风险独立相关。ROC分析显示,ΔPEF识别住院加重的最佳临界值为49 L/min(较基线为27%),敏感性和特异性分别为82.7%和76.7%(曲线下面积[AUC] = 0.872 (95% CI 0.80-0.944, p < 0.05)。ΔCAT评分识别住院加重的最佳临界值为10.5(比基线高63%),敏感性和特异性分别为67.3%和77.4% [AUC]=0.763 (95% CI 0.67 ~ 0.857, p < 0.05)。ΔPEF和ΔCAT联合识别住院加重的AUC为0.900 (95% CI 0.841-0.959, p < 0.05),大于ΔCAT或ΔPEF。结论:ΔPEF和ΔCAT与住院恶化风险独立相关。与CAT相比,PEF在诊断住院加重方面优于CAT。PEF和CAT联合识别比单独使用PEF或CAT更有效。这些结果有助于评估COPD恶化的严重程度,并为临床决策提供有价值的信息。
期刊介绍:
Chronic Respiratory Disease is a peer-reviewed, open access, scholarly journal, created in response to the rising incidence of chronic respiratory diseases worldwide. It publishes high quality research papers and original articles that have immediate relevance to clinical practice and its multi-disciplinary perspective reflects the nature of modern treatment. The journal provides a high quality, multi-disciplinary focus for the publication of original papers, reviews and commentary in the broad area of chronic respiratory disease, particularly its treatment and management.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


