Julia Berman, Victoria Furer, Mark Berman, Ofer Isakov, Devy Zisman, Amir Haddad, Ori Elkayam
{"title":"Treatment with Ixekizumab Following Secukinumab Failure in Patients with Psoriatic Arthritis: Real-Life Experience from a Resistant Population.","authors":"Julia Berman, Victoria Furer, Mark Berman, Ofer Isakov, Devy Zisman, Amir Haddad, Ori Elkayam","doi":"10.2147/BTT.S326792","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To assess the clinical response to ixekizumab following secukinumab failure in patients with psoriatic arthritis.</p><p><strong>Methods: </strong>A retrospective multi-center observational study included psoriatic arthritis (PsA) patients with a history of treatment with secukinumab, further treated with ixekizumab. Primary endpoint was primary response to treatment (drug survival > 6 months); secondary endpoints were changes in disease activity indices from initiation of ixekizumab to 6 and 12 months later and overall drug survival.</p><p><strong>Results: </strong>Of 23 PsA patients, 86% (n = 20) received more than two TNF inhibitors (TNFi). Median secukinumab treatment time was 15 months (IQR 10-21.5 months). Subsequently, 19 patients (83%) had a primary response to ixekizumab. Overall treatment duration during follow-up period for primary responders was 14 months (IQR 10-20.5). Reasons for ixekizumab cessation were worsening psoriasis (27%), peripheral arthritis (27%), both (47%), worsening of axial disease (13%), and adverse events (6%). Articular disease indices including Disease Activity Index for Psoriatic Arthritis (DAPSA), tender joints count (TJC) and Simplified Disease Activity Index (SDAI) were significantly lower at 6 and 12 months (DAPSA 1.5-2 levels reduction; p = 0.018 and 1-1.5 levels reduction; p = 0.031, respectively; TJC -2.16 [-4.0, -0.3]; p = 0.025 and -1.69 [-3.09, -0.28]; p = 0.022, respectively; SDAI -10.13 [-16.4, -3.8], p = 0.003 and -12.2 [-17.1, -7.2], p = 0.0002, respectively). PASI75 at 6 and 12 months was achieved by 63% and 57%, respectively, and PASI100 at 6 and 12 months by 31% and 21%, respectively.</p><p><strong>Conclusion: </strong>Patients with resistant PsA, including inadequate response to secukinumab, demonstrated a good response to ixekizumab, albeit limited on time. Within class switch from secukinumab to ixekizumab may be a plausible therapeutic option in PsA patients following secukinumab failure.</p>","PeriodicalId":9025,"journal":{"name":"Biologics : Targets & Therapy","volume":" ","pages":"463-470"},"PeriodicalIF":3.4000,"publicationDate":"2021-11-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/98/d3/btt-15-463.PMC8608411.pdf","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Biologics : Targets & Therapy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/BTT.S326792","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 6
Abstract
Objective: To assess the clinical response to ixekizumab following secukinumab failure in patients with psoriatic arthritis.
Methods: A retrospective multi-center observational study included psoriatic arthritis (PsA) patients with a history of treatment with secukinumab, further treated with ixekizumab. Primary endpoint was primary response to treatment (drug survival > 6 months); secondary endpoints were changes in disease activity indices from initiation of ixekizumab to 6 and 12 months later and overall drug survival.
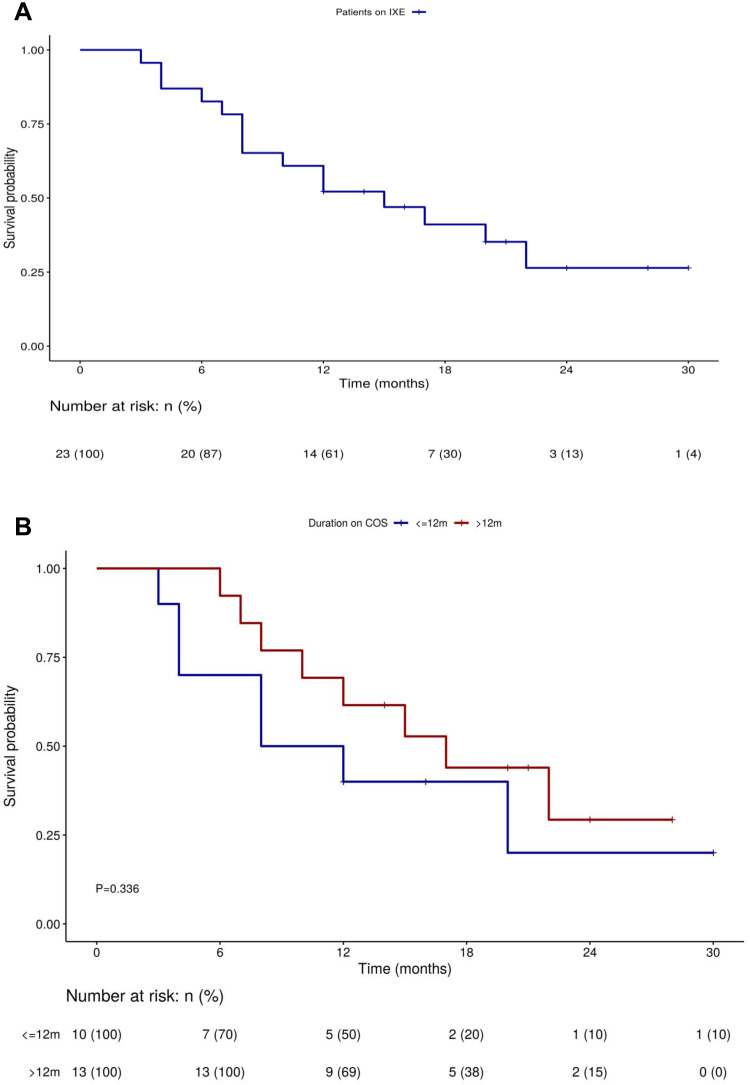
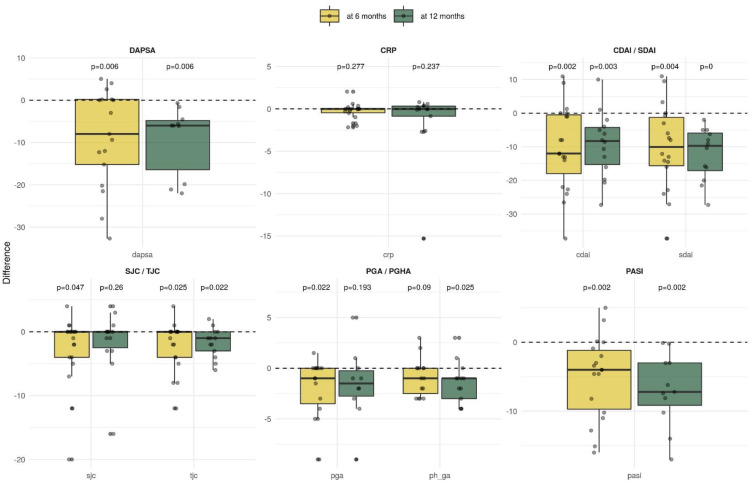
Results: Of 23 PsA patients, 86% (n = 20) received more than two TNF inhibitors (TNFi). Median secukinumab treatment time was 15 months (IQR 10-21.5 months). Subsequently, 19 patients (83%) had a primary response to ixekizumab. Overall treatment duration during follow-up period for primary responders was 14 months (IQR 10-20.5). Reasons for ixekizumab cessation were worsening psoriasis (27%), peripheral arthritis (27%), both (47%), worsening of axial disease (13%), and adverse events (6%). Articular disease indices including Disease Activity Index for Psoriatic Arthritis (DAPSA), tender joints count (TJC) and Simplified Disease Activity Index (SDAI) were significantly lower at 6 and 12 months (DAPSA 1.5-2 levels reduction; p = 0.018 and 1-1.5 levels reduction; p = 0.031, respectively; TJC -2.16 [-4.0, -0.3]; p = 0.025 and -1.69 [-3.09, -0.28]; p = 0.022, respectively; SDAI -10.13 [-16.4, -3.8], p = 0.003 and -12.2 [-17.1, -7.2], p = 0.0002, respectively). PASI75 at 6 and 12 months was achieved by 63% and 57%, respectively, and PASI100 at 6 and 12 months by 31% and 21%, respectively.
Conclusion: Patients with resistant PsA, including inadequate response to secukinumab, demonstrated a good response to ixekizumab, albeit limited on time. Within class switch from secukinumab to ixekizumab may be a plausible therapeutic option in PsA patients following secukinumab failure.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


