Amy May Lin Quek, Delicia Shu Qin Ooi, Ooiean Teng, Chang Yien Chan, Geelyn Jeng Lin Ng, Mei Yen Ng, Sidney Yee, Ee Wan Cheong, Ruifen Weng, Alex R. Cook, Mikael Hartman, Veronique Angeli, Paul Anantharajah Tambyah, Raymond Chee Seong Seet
{"title":"Zinc and vitamin C intake increases spike and neutralising antibody production following SARS-CoV-2 infection","authors":"Amy May Lin Quek, Delicia Shu Qin Ooi, Ooiean Teng, Chang Yien Chan, Geelyn Jeng Lin Ng, Mei Yen Ng, Sidney Yee, Ee Wan Cheong, Ruifen Weng, Alex R. Cook, Mikael Hartman, Veronique Angeli, Paul Anantharajah Tambyah, Raymond Chee Seong Seet","doi":"10.1002/ctm2.731","DOIUrl":null,"url":null,"abstract":"<p>Previous studies have not examined whether pharmacologic interventions could increase SARS-CoV-2 antibody responses. Certain medications (e.g. zinc and vitamin C) are known to stimulate immunologic responses following infections.<span><sup>1, 2</sup></span> Zinc exerts pluripotent effects on the immune system and supports the integrity of the epithelial cell barriers,<span><sup>1, 3</sup></span> while vitamin C is an antioxidant that potentially protects against viral respiratory infections.<span><sup>2</sup></span> Hydroxychloroquine and ivermectin are anti-parasitic medications that are known to modulate innate and adaptive immunity.<span><sup>4, 5</sup></span> By contrast, povidone-iodine is a topical broad spectrum antiseptic capable of direct virucidal effects.<span><sup>6</sup></span> We hypothesise that interventions that support immune regulatory functions could enhance production of anti-SARS-CoV-2 spike and neutralising antibodies among individuals with prior infection. Using materials and resources of the DORM trial (NCT04446104),<span><sup>7</sup></span> we compared the antibody responses at baseline and on day 42 among seropositive participants who received the different medications as part of this trial.</p><p>Participants from the study were selected from the DORM trial, an open label, randomised clinical trial that examined the efficacy of either oral hydroxychloroquine (400 mg followed by 200 mg/day), povidone-iodine throat spray (three times a day, approximately 270 μg/day), oral ivermectin (12 mg, single dose), oral zinc + vitamin C (80 mg zinc sulfate, 500 mg vitamin C/day) or oral vitamin C (500 mg/day), for 42 days to reduce SARS-CoV-2 infection (Supporting Information).<span><sup>7</sup></span> From 4257 recruited participants, those found with new SARS-CoV-2 infection on recruitment were enrolled into the present substudy.</p><p>Antibody titers were measured using two different assays that quantified binding (Elecsys®, Roche, Germany) and neutralising antibodies (cPass™, GenScript, USA) targeting the SARS-CoV-2 spike antigens. To examine the impact of different interventions on the immune cells, the frequency of B and T lymphocytes was analysed using pre-formulated DURAClone IM Phenotyping Basic and B Cell Panels (Beckman, USA). Serum zinc was measured in zinc-treated participants using an inductively coupled plasma mass spectrometry method (PerkinElmer, USA). SPSS Statistics version 27 (IBM Corporation, Armonk, USA) was used for all analysis (Supporting Information).</p><p>A total of 422 men were enrolled, from among 478 seropositive cases in the DORM trial; those excluded either withdrew from the study (<i>n</i> = 22) or did not return for follow-up visit (<i>n</i> = 24) (Figure S1). The primary cohort comprised 422 men (mean age, 33.0 years; standard deviation (SD), 7.3 years) who received zinc + vitamin C (<i>n</i> = 68), hydroxychloroquine (<i>n</i> = 67), ivermectin (<i>n</i> = 99), povidone-iodine (<i>n</i> = 107) and vitamin C (<i>n</i> = 81) (Table 1, Figure S1). Few had medical co-morbidities (hypertension, 1.4%; diabetes mellitus, 0.7%; hyperlipidemia, 0.2%). Overall, anti-SARS-CoV-2 spike antibody positivity increased from baseline level of 80% to 94% by day 42, whereas neutralising antibody positivity increased from 44% to 49% by day 42.</p><p>Anti-SARS-CoV-2 immunoglobulin G (IgG) levels, which were comparable at baseline, increased substantially by day 42, especially in the zinc + vitamin C group compared with other interventions (Figure 1A,B). By contrast, an increase in neutralising antibodies (measured by percent inhibition of surrogate virus neutralisation tests) was confined to the zinc + vitamin C group by day 42 (Figure 1C,D). Among seropositive men without neutralising antibodies at study entry, conversion to neutralising antibody positivity was highest in the zinc + vitamin C group (46.7%) by day 42, compared with vitamin C (19.6%), hydroxychloroquine (30.8%), ivermectin (20%) and povidone-iodine (9.8%) (<i>p</i> < .001, chi-squared test) (Figure 2). Overall, seropositive men who were initially negative for neutralising antibodies were approximately four times more likely to develop neutralising antibody positivity by day 42 in the zinc + vitamin C group compared with other interventions (odds ratio (OR) 3.75, 95% confidence interval (CI) 1.69–8.32). To further investigate the primary findings, zinc was measured in baseline and day 42 sera of men who received zinc + vitamin C. As expected, serum zinc rose from a baseline mean of 14.0 mmol/l (SD 1.9) to 17.8 mmol/l (SD 2.5) by day 42. The extent of rise in serum zinc from baseline to day 42 correlated significantly with anti-SARS-CoV-2 spike IgG (<i>r</i> = 0.401, <i>p</i> = .001) (Figure 3A), but not with neutralising antibodies (Figure 3B).</p><p>To examine the impact of the different interventions on immune cell populations, immunophenotyping was performed on whole blood in 211 participants (Figure S2). Compared with other interventions, zinc + vitamin C-treated men had a higher percentage of transitional B cells (mean 3.49% vs. 2.54%, <i>p</i> < .001) (Table S1). No statistically significant differences were observed with isotype class switch, marginal zone, naïve and plasmablast B cells, CD4+ T cells, CD8+ T cells, natural killer cells, classical, intermediate and non-classical monocytes. In this cohort, transitional B cells were weakly correlated with neutralising antibodies (<i>r</i> = 0.192, <i>p</i> = .005) (Figure S3A). Among men who were initially negative for neutralising antibodies, an increase in double-negative T cells frequency was observed among those with seroconversion in neutralising antibodies by day 42 (mean 8.40% vs. 5.92%, <i>p</i> = .004) (Table S2). A weak but statistically significant association was observed between double-negative T cells and neutralising antibodies by day 42 (<i>r</i> = 0.272, <i>p</i> = .004) (Figure S3B).</p><p>Findings from this study highlight suboptimal production of neutralising antibodies in more than 50% of individuals following an asymptomatic infection. Compared with other interventions, those who received zinc + vitamin C were found to subsequently mount a greater antibody response. Among individuals who were initially seronegative to neutralising antibodies at study entry, conversion to positivity was approximately four times higher among zinc-treated men compared with those who received other interventions. By activating innate and adaptive B and T cellular responses, the immune system produces binding antibodies especially against the nucleocapsid and spike proteins of the SARS-CoV-2 virus, and neutralising antibodies to aid immunity.<span><sup>8, 9</sup></span> We observed significant alterations in early transitional B cells but not in B cell populations at later stages of maturation. The significance of increase in double-negative T cells among neutralising antibody seroconverters is unclear. Among hospitalised patients, those with a higher double-negative T cells to surface expression of CD4 and CD8, tended to have a milder disease with fewer requiring oxygen and ventilatory support,<span><sup>10</sup></span> suggesting double-negative T cells could be beneficial during SARS-CoV-2 infection.</p><p>To our knowledge, this study is the first to demonstrate the efficacy of oral zinc + vitamin C treatment to stimulate antibody production following SARS-CoV-2 infection. Future studies should examine whether increase in antibody production following zinc + vitamin C could sustain immunity against re-infection, and enhance antibody responses following vaccination among immunocompromised individuals. Results from this study should be confirmed in prospectively designed studies.</p><p>Dr. Seet reported receiving grants from the National Medical Research Council and Temasek Foundation, Singapore. Dr. Tambyah reported receiving grants from Johnson and Johnson, GlaxoSmithKline and Roche.</p>","PeriodicalId":10189,"journal":{"name":"Clinical and Translational Medicine","volume":"12 2","pages":""},"PeriodicalIF":7.9000,"publicationDate":"2022-02-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8858613/pdf/","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ctm2.731","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, RESEARCH & EXPERIMENTAL","Score":null,"Total":0}
引用次数: 8
Abstract
Previous studies have not examined whether pharmacologic interventions could increase SARS-CoV-2 antibody responses. Certain medications (e.g. zinc and vitamin C) are known to stimulate immunologic responses following infections.1, 2 Zinc exerts pluripotent effects on the immune system and supports the integrity of the epithelial cell barriers,1, 3 while vitamin C is an antioxidant that potentially protects against viral respiratory infections.2 Hydroxychloroquine and ivermectin are anti-parasitic medications that are known to modulate innate and adaptive immunity.4, 5 By contrast, povidone-iodine is a topical broad spectrum antiseptic capable of direct virucidal effects.6 We hypothesise that interventions that support immune regulatory functions could enhance production of anti-SARS-CoV-2 spike and neutralising antibodies among individuals with prior infection. Using materials and resources of the DORM trial (NCT04446104),7 we compared the antibody responses at baseline and on day 42 among seropositive participants who received the different medications as part of this trial.
Participants from the study were selected from the DORM trial, an open label, randomised clinical trial that examined the efficacy of either oral hydroxychloroquine (400 mg followed by 200 mg/day), povidone-iodine throat spray (three times a day, approximately 270 μg/day), oral ivermectin (12 mg, single dose), oral zinc + vitamin C (80 mg zinc sulfate, 500 mg vitamin C/day) or oral vitamin C (500 mg/day), for 42 days to reduce SARS-CoV-2 infection (Supporting Information).7 From 4257 recruited participants, those found with new SARS-CoV-2 infection on recruitment were enrolled into the present substudy.
Antibody titers were measured using two different assays that quantified binding (Elecsys®, Roche, Germany) and neutralising antibodies (cPass™, GenScript, USA) targeting the SARS-CoV-2 spike antigens. To examine the impact of different interventions on the immune cells, the frequency of B and T lymphocytes was analysed using pre-formulated DURAClone IM Phenotyping Basic and B Cell Panels (Beckman, USA). Serum zinc was measured in zinc-treated participants using an inductively coupled plasma mass spectrometry method (PerkinElmer, USA). SPSS Statistics version 27 (IBM Corporation, Armonk, USA) was used for all analysis (Supporting Information).
A total of 422 men were enrolled, from among 478 seropositive cases in the DORM trial; those excluded either withdrew from the study (n = 22) or did not return for follow-up visit (n = 24) (Figure S1). The primary cohort comprised 422 men (mean age, 33.0 years; standard deviation (SD), 7.3 years) who received zinc + vitamin C (n = 68), hydroxychloroquine (n = 67), ivermectin (n = 99), povidone-iodine (n = 107) and vitamin C (n = 81) (Table 1, Figure S1). Few had medical co-morbidities (hypertension, 1.4%; diabetes mellitus, 0.7%; hyperlipidemia, 0.2%). Overall, anti-SARS-CoV-2 spike antibody positivity increased from baseline level of 80% to 94% by day 42, whereas neutralising antibody positivity increased from 44% to 49% by day 42.
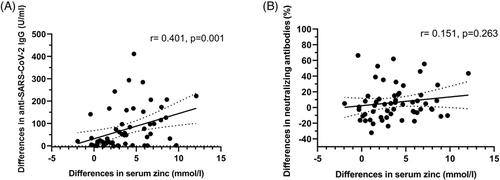
Anti-SARS-CoV-2 immunoglobulin G (IgG) levels, which were comparable at baseline, increased substantially by day 42, especially in the zinc + vitamin C group compared with other interventions (Figure 1A,B). By contrast, an increase in neutralising antibodies (measured by percent inhibition of surrogate virus neutralisation tests) was confined to the zinc + vitamin C group by day 42 (Figure 1C,D). Among seropositive men without neutralising antibodies at study entry, conversion to neutralising antibody positivity was highest in the zinc + vitamin C group (46.7%) by day 42, compared with vitamin C (19.6%), hydroxychloroquine (30.8%), ivermectin (20%) and povidone-iodine (9.8%) (p < .001, chi-squared test) (Figure 2). Overall, seropositive men who were initially negative for neutralising antibodies were approximately four times more likely to develop neutralising antibody positivity by day 42 in the zinc + vitamin C group compared with other interventions (odds ratio (OR) 3.75, 95% confidence interval (CI) 1.69–8.32). To further investigate the primary findings, zinc was measured in baseline and day 42 sera of men who received zinc + vitamin C. As expected, serum zinc rose from a baseline mean of 14.0 mmol/l (SD 1.9) to 17.8 mmol/l (SD 2.5) by day 42. The extent of rise in serum zinc from baseline to day 42 correlated significantly with anti-SARS-CoV-2 spike IgG (r = 0.401, p = .001) (Figure 3A), but not with neutralising antibodies (Figure 3B).
To examine the impact of the different interventions on immune cell populations, immunophenotyping was performed on whole blood in 211 participants (Figure S2). Compared with other interventions, zinc + vitamin C-treated men had a higher percentage of transitional B cells (mean 3.49% vs. 2.54%, p < .001) (Table S1). No statistically significant differences were observed with isotype class switch, marginal zone, naïve and plasmablast B cells, CD4+ T cells, CD8+ T cells, natural killer cells, classical, intermediate and non-classical monocytes. In this cohort, transitional B cells were weakly correlated with neutralising antibodies (r = 0.192, p = .005) (Figure S3A). Among men who were initially negative for neutralising antibodies, an increase in double-negative T cells frequency was observed among those with seroconversion in neutralising antibodies by day 42 (mean 8.40% vs. 5.92%, p = .004) (Table S2). A weak but statistically significant association was observed between double-negative T cells and neutralising antibodies by day 42 (r = 0.272, p = .004) (Figure S3B).
Findings from this study highlight suboptimal production of neutralising antibodies in more than 50% of individuals following an asymptomatic infection. Compared with other interventions, those who received zinc + vitamin C were found to subsequently mount a greater antibody response. Among individuals who were initially seronegative to neutralising antibodies at study entry, conversion to positivity was approximately four times higher among zinc-treated men compared with those who received other interventions. By activating innate and adaptive B and T cellular responses, the immune system produces binding antibodies especially against the nucleocapsid and spike proteins of the SARS-CoV-2 virus, and neutralising antibodies to aid immunity.8, 9 We observed significant alterations in early transitional B cells but not in B cell populations at later stages of maturation. The significance of increase in double-negative T cells among neutralising antibody seroconverters is unclear. Among hospitalised patients, those with a higher double-negative T cells to surface expression of CD4 and CD8, tended to have a milder disease with fewer requiring oxygen and ventilatory support,10 suggesting double-negative T cells could be beneficial during SARS-CoV-2 infection.
To our knowledge, this study is the first to demonstrate the efficacy of oral zinc + vitamin C treatment to stimulate antibody production following SARS-CoV-2 infection. Future studies should examine whether increase in antibody production following zinc + vitamin C could sustain immunity against re-infection, and enhance antibody responses following vaccination among immunocompromised individuals. Results from this study should be confirmed in prospectively designed studies.
Dr. Seet reported receiving grants from the National Medical Research Council and Temasek Foundation, Singapore. Dr. Tambyah reported receiving grants from Johnson and Johnson, GlaxoSmithKline and Roche.
同型分类开关、边缘区、naïve和浆母细胞B细胞、CD4+ T细胞、CD8+ T细胞、自然杀伤细胞、经典、中间和非经典单核细胞的差异均无统计学意义。在该队列中,移行性B细胞与中和抗体呈弱相关(r = 0.192, p = 0.005)(图S3A)。在最初中和抗体阴性的男性中,在第42天中和抗体血清转化的男性中观察到双阴性T细胞频率增加(平均8.40% vs. 5.92%, p = 0.004)(表S2)。在第42天,双阴性T细胞和中和抗体之间存在微弱但有统计学意义的关联(r = 0.272, p = 0.004)(图S3B)。这项研究的结果强调,在无症状感染后,超过50%的个体产生了次优的中和抗体。与其他干预措施相比,接受锌+维生素C治疗的患者随后产生了更大的抗体反应。在研究开始时对中和抗体最初血清阴性的个体中,锌治疗的男性转化为阳性的几率大约是接受其他干预的男性的四倍。通过激活先天和适应性B细胞和T细胞反应,免疫系统产生结合抗体,特别是针对SARS-CoV-2病毒的核衣壳和刺突蛋白,并中和抗体以帮助免疫。8,9我们观察到在早期过渡性B细胞中有显著的改变,但在成熟后期的B细胞群中没有。在中和抗体血清转换者中双阴性T细胞增加的意义尚不清楚。在住院患者中,CD4和CD8表面双阴性T细胞表达较高的患者往往病情较轻,需要的氧气和呼吸支持较少,10表明双阴性T细胞在SARS-CoV-2感染期间可能是有益的。据我们所知,这项研究首次证明了口服锌+维生素C治疗刺激SARS-CoV-2感染后抗体产生的有效性。未来的研究应该研究锌+维生素C后抗体产生的增加是否可以维持免疫系统免受再次感染,并增强免疫功能低下个体接种疫苗后的抗体反应。本研究的结果应在前瞻性设计的研究中得到证实。Seet报告说,他获得了新加坡国家医学研究委员会和淡马锡基金会的资助。Tambyah博士报告接受了强生、葛兰素史克和罗氏的资助。
期刊介绍:
Clinical and Translational Medicine (CTM) is an international, peer-reviewed, open-access journal dedicated to accelerating the translation of preclinical research into clinical applications and fostering communication between basic and clinical scientists. It highlights the clinical potential and application of various fields including biotechnologies, biomaterials, bioengineering, biomarkers, molecular medicine, omics science, bioinformatics, immunology, molecular imaging, drug discovery, regulation, and health policy. With a focus on the bench-to-bedside approach, CTM prioritizes studies and clinical observations that generate hypotheses relevant to patients and diseases, guiding investigations in cellular and molecular medicine. The journal encourages submissions from clinicians, researchers, policymakers, and industry professionals.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


