Muhammad B Darwish, Shankar I Logarajah, Kei Nagatomo, Terence Jackson, Annie Laurie Benzie, Patrick James McLaren, Edward Cho, Houssam Osman, D Rohan Jeyarajah
{"title":"To Wrap or Not to Wrap After Heller Myotomy.","authors":"Muhammad B Darwish, Shankar I Logarajah, Kei Nagatomo, Terence Jackson, Annie Laurie Benzie, Patrick James McLaren, Edward Cho, Houssam Osman, D Rohan Jeyarajah","doi":"10.4293/JSLS.2021.00054","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and objectives: </strong>The primary aim of this study is to assess the necessity of fundoplication for reflux in patients undergoing Heller myotomy for achalasia. The secondary aim is to assess the safety of the robotic approach to Heller myotomy.</p><p><strong>Methods: </strong>This is a single institution, retrospective analysis of 61 patients who underwent robotic Heller myotomy with or without fundoplication over a 4-year period (January 1, 2015 - December 31, 2019). Symptoms were evaluated using pre-operative and postoperative Eckardt scores at < 2 weeks (short-term) and 4 - 55 months (long-term) postoperatively. Incidence of gastroesophageal reflux and use of antacids postoperatively were assessed. Long-term patient satisfaction and quality of life (QOL) were assessed with a phone survey. Finally, the perioperative safety profile of robotic Heller myotomy was evaluated.</p><p><strong>Results: </strong>The long-term average Eckardt score in patients undergoing Heller myotomy without fundoplication was notably lower than in patients with a fundoplication (0.72 vs 2.44). Gastroesophageal reflux rates were lower in patient without a fundoplication (16.0% vs 33.3%). Additionally, dysphagia rates were lower in patients without a fundoplication (32.0% vs 44.4%). Only 34.8% (8/25) of patients without fundoplication continued use of antacids in the long-term. There were no mortalities and a 4.2% complication rate with two delayed leaks.</p><p><strong>Conclusion: </strong>Robotic Heller myotomy without fundoplication is safe and effective for achalasia. The rate of reflux symptoms and overall Eckardt scores were low postoperatively. Great patient satisfaction and QOL were observed in the long term. Our results suggest that fundoplication is unnecessary when performing Heller myotomy.</p>","PeriodicalId":17679,"journal":{"name":"JSLS : Journal of the Society of Laparoendoscopic Surgeons","volume":"25 4","pages":""},"PeriodicalIF":1.4000,"publicationDate":"2021-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fa/1f/e2021.00054.PMC8580166.pdf","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JSLS : Journal of the Society of Laparoendoscopic Surgeons","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4293/JSLS.2021.00054","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 1
Abstract
Background and objectives: The primary aim of this study is to assess the necessity of fundoplication for reflux in patients undergoing Heller myotomy for achalasia. The secondary aim is to assess the safety of the robotic approach to Heller myotomy.
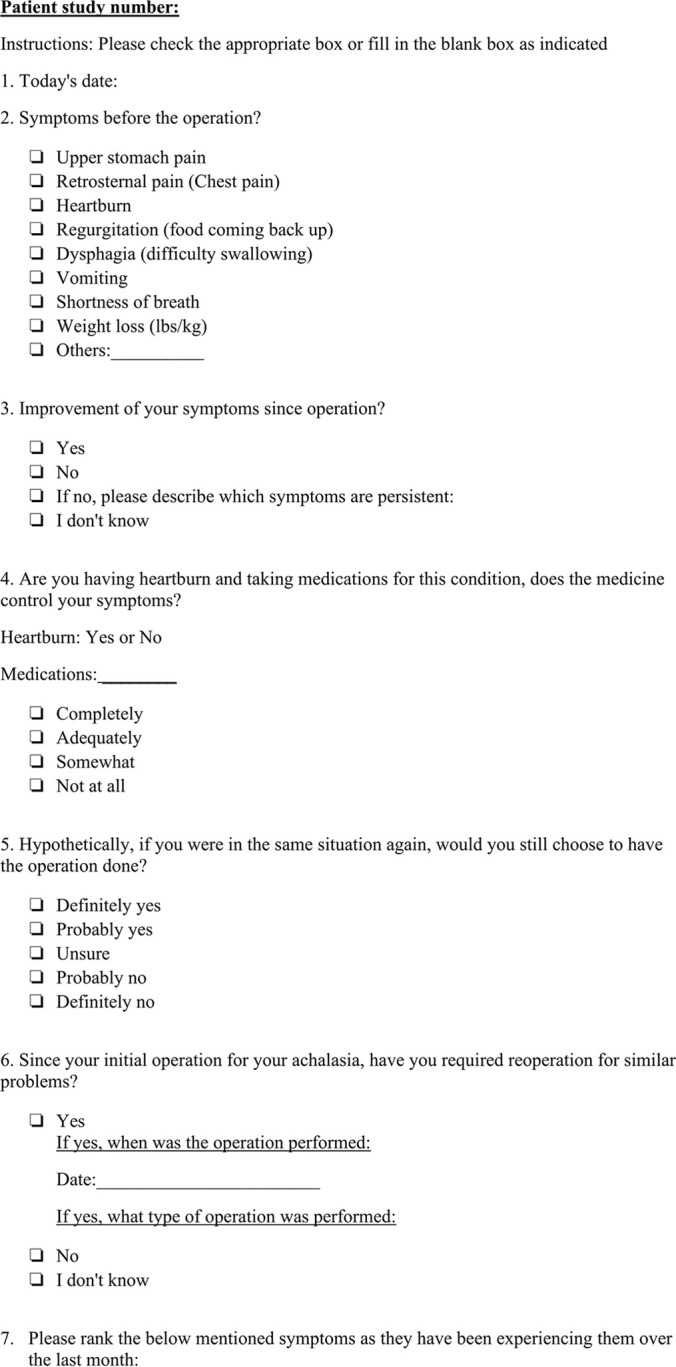
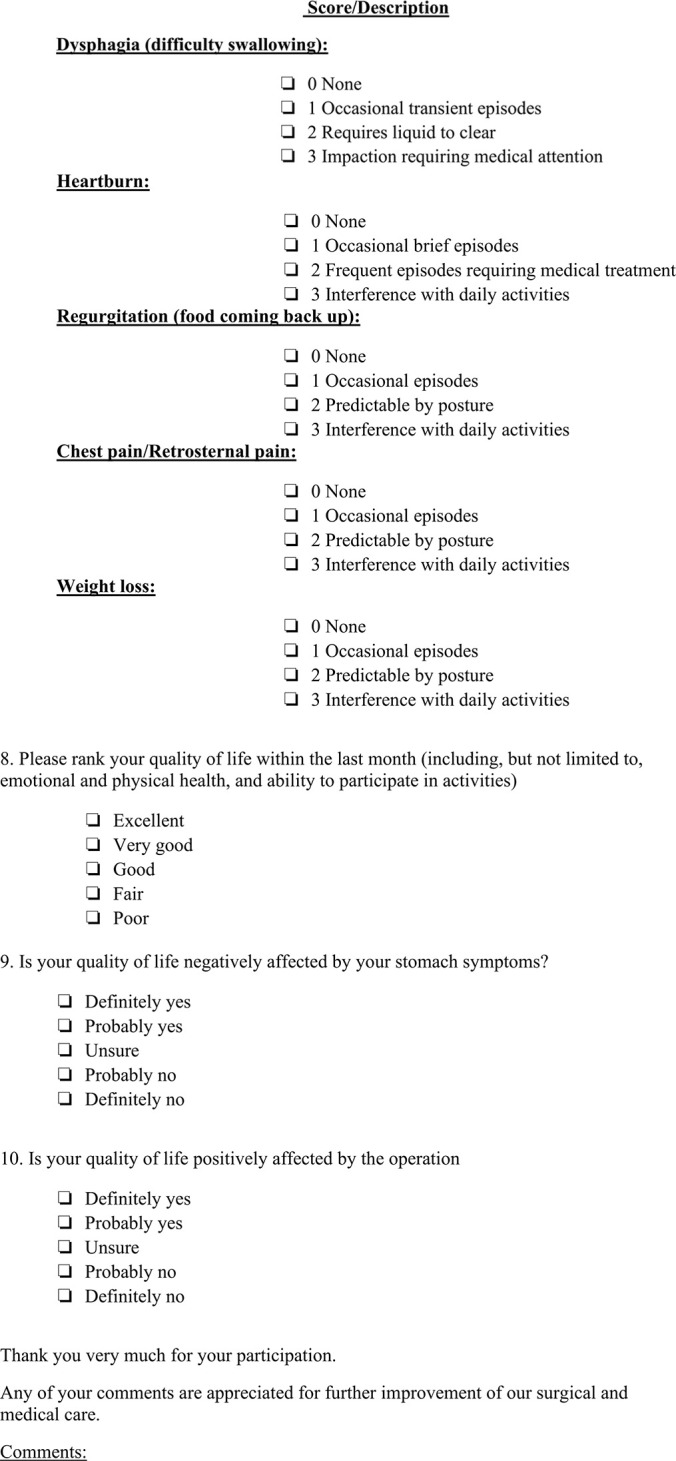
Methods: This is a single institution, retrospective analysis of 61 patients who underwent robotic Heller myotomy with or without fundoplication over a 4-year period (January 1, 2015 - December 31, 2019). Symptoms were evaluated using pre-operative and postoperative Eckardt scores at < 2 weeks (short-term) and 4 - 55 months (long-term) postoperatively. Incidence of gastroesophageal reflux and use of antacids postoperatively were assessed. Long-term patient satisfaction and quality of life (QOL) were assessed with a phone survey. Finally, the perioperative safety profile of robotic Heller myotomy was evaluated.
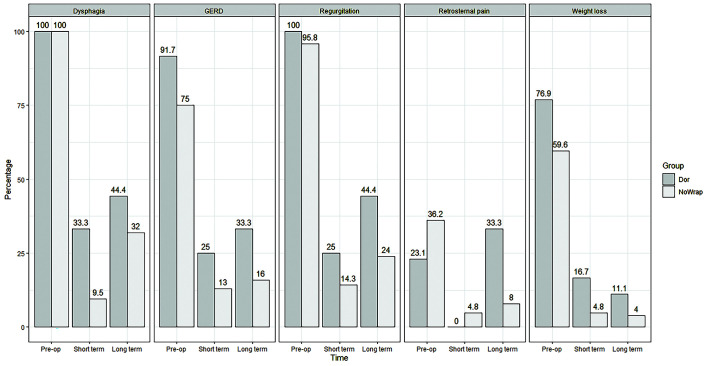
Results: The long-term average Eckardt score in patients undergoing Heller myotomy without fundoplication was notably lower than in patients with a fundoplication (0.72 vs 2.44). Gastroesophageal reflux rates were lower in patient without a fundoplication (16.0% vs 33.3%). Additionally, dysphagia rates were lower in patients without a fundoplication (32.0% vs 44.4%). Only 34.8% (8/25) of patients without fundoplication continued use of antacids in the long-term. There were no mortalities and a 4.2% complication rate with two delayed leaks.
Conclusion: Robotic Heller myotomy without fundoplication is safe and effective for achalasia. The rate of reflux symptoms and overall Eckardt scores were low postoperatively. Great patient satisfaction and QOL were observed in the long term. Our results suggest that fundoplication is unnecessary when performing Heller myotomy.
背景和目的:本研究的主要目的是评估接受Heller肌切开术治疗贲门失弛缓症患者反流的必要性。第二个目的是评估机器人入路海勒肌切开术的安全性。方法:这是一项单一机构的回顾性分析,在4年期间(2015年1月1日至2019年12月31日),61名患者接受了机器人Heller肌切开术,伴有或不伴有眼底复制。在术后< 2周(短期)和4 - 55个月(长期)使用术前和术后Eckardt评分评估症状。评估胃食管反流发生率及术后抗酸药使用情况。通过电话调查评估患者的长期满意度和生活质量。最后,对机器人Heller肌切开术的围手术期安全性进行评价。结果:行Heller肌切开术无底重复患者的长期平均Eckardt评分明显低于有底重复患者(0.72 vs 2.44)。胃食管反流率在没有胃底重叠的患者中较低(16.0% vs 33.3%)。此外,没有基底部复制的患者的吞咽困难发生率较低(32.0% vs 44.4%)。只有34.8%(8/25)的无底溃患者继续长期使用抗酸药。无死亡,2例迟发性漏的并发症发生率为4.2%。结论:机器人Heller肌切开术治疗贲门失弛缓症安全有效。术后反流症状发生率和总Eckardt评分均较低。长期观察患者满意度和生活质量。我们的结果表明,在进行Heller肌切开术时,不需要重复眼底。
期刊介绍:
JSLS, Journal of the Society of Laparoscopic & Robotic Surgeons publishes original scientific articles on basic science and technical topics in all the fields involved with laparoscopic, robotic, and minimally invasive surgery. CRSLS, MIS Case Reports from SLS is dedicated to the publication of Case Reports in the field of minimally invasive surgery. The journals seek to advance our understandings and practice of minimally invasive, image-guided surgery by providing a forum for all relevant disciplines and by promoting the exchange of information and ideas across specialties.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


