Identification and validation of objective triggers for initiation of resuscitation management of acutely ill non-trauma patients: the INITIATE IRON MAN study.
Alexandros Rovas, Efe Paracikoglu, Mark Michael, André Gries, Janina Dziegielewski, Hermann Pavenstädt, Michael Bernhard, Philipp Kümpers
{"title":"Identification and validation of objective triggers for initiation of resuscitation management of acutely ill non-trauma patients: the INITIATE IRON MAN study.","authors":"Alexandros Rovas, Efe Paracikoglu, Mark Michael, André Gries, Janina Dziegielewski, Hermann Pavenstädt, Michael Bernhard, Philipp Kümpers","doi":"10.1186/s13049-021-00973-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>While there are clear national resuscitation room admission guidelines for major trauma patients, there are no comparable alarm criteria for critically ill nontrauma (CINT) patients in the emergency department (ED). The aim of this study was to define and validate specific trigger factor cut-offs for identification of CINT patients in need of a structured resuscitation management protocol.</p><p><strong>Methods: </strong>All CINT patients at a German university hospital ED for whom structured resuscitation management would have been deemed desirable were prospectively enrolled over a 6-week period (derivation cohort, n = 108). The performance of different thresholds and/or combinations of trigger factors immediately available during triage were compared with the National Early Warning Score (NEWS) and Quick Sequential Organ Failure Assessment (qSOFA) score. Identified combinations were then tested in a retrospective sample of consecutive nontrauma patients presenting at the ED during a 4-week period (n = 996), and two large external datasets of CINT patients treated in two German university hospital EDs (validation cohorts 1 [n = 357] and 2 [n = 187]).</p><p><strong>Results: </strong>The any-of-the-following trigger factor iteration with the best performance in the derivation cohort included: systolic blood pressure < 90 mmHg, oxygen saturation < 90%, and Glasgow Coma Scale score < 15 points. This set of triggers identified > 80% of patients in the derivation cohort and performed better than NEWS and qSOFA scores in the internal validation cohort (sensitivity = 98.5%, specificity = 98.6%). When applied to the external validation cohorts, need for advanced resuscitation measures and hospital mortality (6.7 vs. 28.6%, p < 0.0001 and 2.7 vs. 20.0%, p < 0.012) were significantly lower in trigger factor-negative patients.</p><p><strong>Conclusion: </strong>Our simple, any-of-the-following decision rule can serve as an objective trigger for initiating resuscitation room management of CINT patients in the ED.</p>","PeriodicalId":501057,"journal":{"name":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","volume":" ","pages":"160"},"PeriodicalIF":0.0000,"publicationDate":"2021-11-13","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8590263/pdf/","citationCount":"7","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scandinavian Journal of Trauma, Resuscitation and Emergency Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13049-021-00973-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 7
Abstract
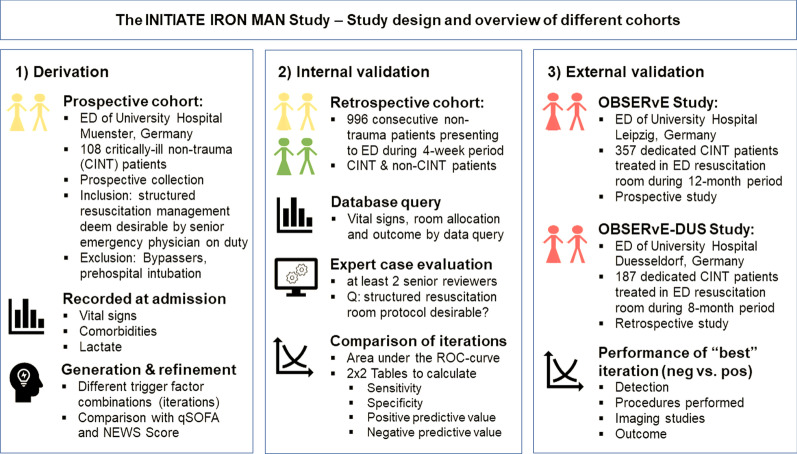
Background: While there are clear national resuscitation room admission guidelines for major trauma patients, there are no comparable alarm criteria for critically ill nontrauma (CINT) patients in the emergency department (ED). The aim of this study was to define and validate specific trigger factor cut-offs for identification of CINT patients in need of a structured resuscitation management protocol.
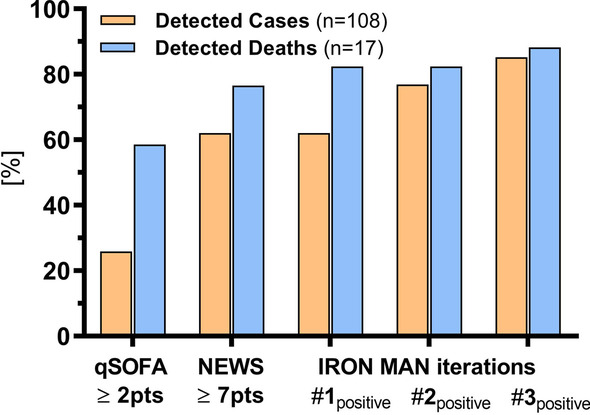
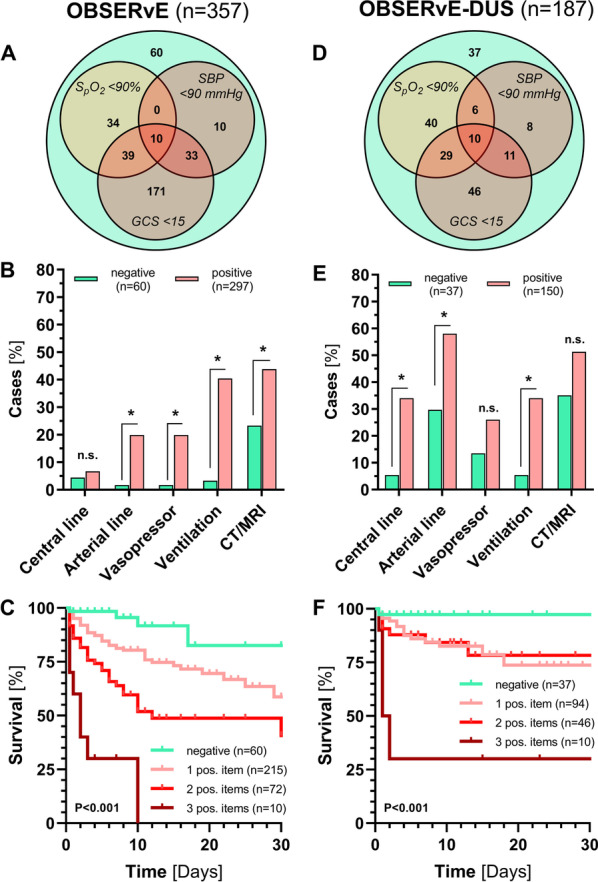
Methods: All CINT patients at a German university hospital ED for whom structured resuscitation management would have been deemed desirable were prospectively enrolled over a 6-week period (derivation cohort, n = 108). The performance of different thresholds and/or combinations of trigger factors immediately available during triage were compared with the National Early Warning Score (NEWS) and Quick Sequential Organ Failure Assessment (qSOFA) score. Identified combinations were then tested in a retrospective sample of consecutive nontrauma patients presenting at the ED during a 4-week period (n = 996), and two large external datasets of CINT patients treated in two German university hospital EDs (validation cohorts 1 [n = 357] and 2 [n = 187]).
Results: The any-of-the-following trigger factor iteration with the best performance in the derivation cohort included: systolic blood pressure < 90 mmHg, oxygen saturation < 90%, and Glasgow Coma Scale score < 15 points. This set of triggers identified > 80% of patients in the derivation cohort and performed better than NEWS and qSOFA scores in the internal validation cohort (sensitivity = 98.5%, specificity = 98.6%). When applied to the external validation cohorts, need for advanced resuscitation measures and hospital mortality (6.7 vs. 28.6%, p < 0.0001 and 2.7 vs. 20.0%, p < 0.012) were significantly lower in trigger factor-negative patients.
Conclusion: Our simple, any-of-the-following decision rule can serve as an objective trigger for initiating resuscitation room management of CINT patients in the ED.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


