Optimizing responsiveness to feedback about antibiotic prescribing in primary care: protocol for two interrelated randomized implementation trials with embedded process evaluations.
Jennifer Shuldiner, Kevin L Schwartz, Bradley J Langford, Noah M Ivers
{"title":"Optimizing responsiveness to feedback about antibiotic prescribing in primary care: protocol for two interrelated randomized implementation trials with embedded process evaluations.","authors":"Jennifer Shuldiner, Kevin L Schwartz, Bradley J Langford, Noah M Ivers","doi":"10.1186/s13012-022-01194-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Audit and feedback (A&F) that shows how health professionals compare to those of their peers, can be an effective intervention to reduce unnecessary antibiotic prescribing among family physicians. However, the most impactful design approach to A&F to achieve this aim is uncertain. We will test three design modifications of antibiotic A&F that could be readily scaled and sustained if shown to be effective: (1) inclusion of case-mix-adjusted peer comparator versus a crude comparator, (2) emphasizing harms, rather than lack of benefits, and (3) providing a viral prescription pad.</p><p><strong>Methods: </strong>We will conduct two interrelated pragmatic randomized trials in January 2021. One trial will include family physicians in Ontario who have signed up to receive their MyPractice: Primary Care report from Ontario Health (\"OH Trial\"). These physicians will be cluster-randomized by practice, 1:1 to intervention or control. The intervention group will also receive a Viral Prescription Pad mailed to their office as well as added emphasis in their report on use of the pad. Ontario family physicians who have not signed up to receive their MyPractice: Primary Care report will be included in the other trial administered by Public Health Ontario (\"PHO Trial\"). These physicians will be allocated 4:1 to intervention or control. The intervention group will be further randomized by two factors: case-mix adjusted versus unadjusted comparator and emphasis or not on harms of antibiotics. Physicians in the intervention arm of this trial will receive one of four versions of a personalized antibiotic A&F letter from PHO. For both trials, the primary outcome is the antibiotic prescribing rate per 1000 patient visits, measured at 6 months post-randomization, the primary analysis will use Poisson regression and we will follow the intention to treat principle. A mixed-methods process evaluation will use surveys and interviews with family physicians to explore potential mechanisms underlying the observed effects, exploring targeted constructs including intention, self-efficacy, outcome expectancies, descriptive norms, and goal prioritization.</p><p><strong>Discussion: </strong>This protocol describes the rationale and methodology of two interrelated pragmatic trials testing variations of theory-informed components of an audit and feedback intervention to determine how to optimize A&F interventions for antibiotic prescribing in primary care.</p><p><strong>Trial registration: </strong>NCT04594200, NCT05044052. CIHR Grant ID: 398514.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"17"},"PeriodicalIF":0.0000,"publicationDate":"2022-02-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8842929/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13012-022-01194-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
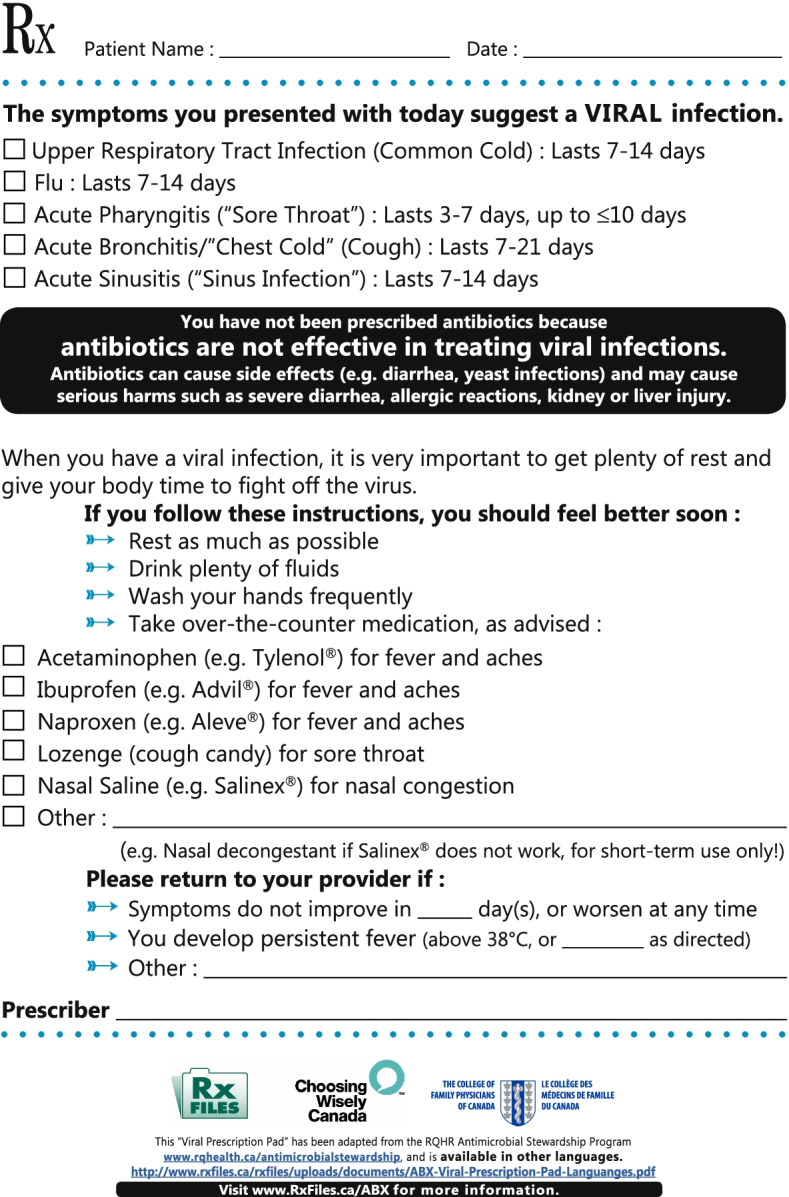
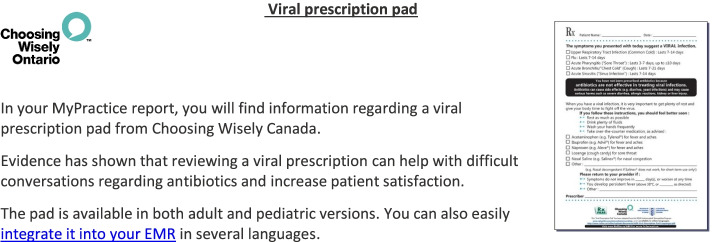
Background: Audit and feedback (A&F) that shows how health professionals compare to those of their peers, can be an effective intervention to reduce unnecessary antibiotic prescribing among family physicians. However, the most impactful design approach to A&F to achieve this aim is uncertain. We will test three design modifications of antibiotic A&F that could be readily scaled and sustained if shown to be effective: (1) inclusion of case-mix-adjusted peer comparator versus a crude comparator, (2) emphasizing harms, rather than lack of benefits, and (3) providing a viral prescription pad.
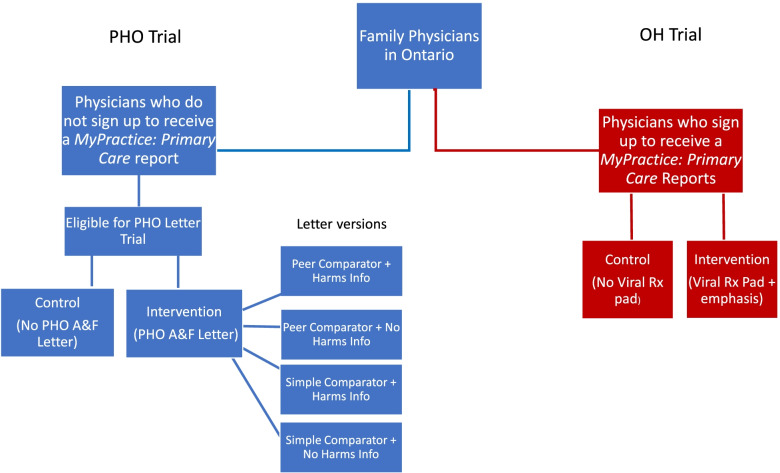
Methods: We will conduct two interrelated pragmatic randomized trials in January 2021. One trial will include family physicians in Ontario who have signed up to receive their MyPractice: Primary Care report from Ontario Health ("OH Trial"). These physicians will be cluster-randomized by practice, 1:1 to intervention or control. The intervention group will also receive a Viral Prescription Pad mailed to their office as well as added emphasis in their report on use of the pad. Ontario family physicians who have not signed up to receive their MyPractice: Primary Care report will be included in the other trial administered by Public Health Ontario ("PHO Trial"). These physicians will be allocated 4:1 to intervention or control. The intervention group will be further randomized by two factors: case-mix adjusted versus unadjusted comparator and emphasis or not on harms of antibiotics. Physicians in the intervention arm of this trial will receive one of four versions of a personalized antibiotic A&F letter from PHO. For both trials, the primary outcome is the antibiotic prescribing rate per 1000 patient visits, measured at 6 months post-randomization, the primary analysis will use Poisson regression and we will follow the intention to treat principle. A mixed-methods process evaluation will use surveys and interviews with family physicians to explore potential mechanisms underlying the observed effects, exploring targeted constructs including intention, self-efficacy, outcome expectancies, descriptive norms, and goal prioritization.
Discussion: This protocol describes the rationale and methodology of two interrelated pragmatic trials testing variations of theory-informed components of an audit and feedback intervention to determine how to optimize A&F interventions for antibiotic prescribing in primary care.
Trial registration: NCT04594200, NCT05044052. CIHR Grant ID: 398514.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


