A randomized crossover study comparing different tacrolimus formulations to reduce intrapatient variability in tacrolimus exposure in kidney transplant recipients.
Kim L W Bunthof, Linda Al-Hassany, Gizal Nakshbandi, Dennis A Hesselink, Ron H N van Schaik, Marc A G J Ten Dam, Marije C Baas, Luuk B Hilbrands, Teun van Gelder
{"title":"A randomized crossover study comparing different tacrolimus formulations to reduce intrapatient variability in tacrolimus exposure in kidney transplant recipients.","authors":"Kim L W Bunthof, Linda Al-Hassany, Gizal Nakshbandi, Dennis A Hesselink, Ron H N van Schaik, Marc A G J Ten Dam, Marije C Baas, Luuk B Hilbrands, Teun van Gelder","doi":"10.1111/cts.13206","DOIUrl":null,"url":null,"abstract":"<p><p>A high intrapatient variability (IPV) in tacrolimus exposure is a risk factor for poor long-term outcomes after kidney transplantation. The main objective of this trial was to investigate whether tacrolimus IPV decreases after switching patients from immediate-release (IR)-tacrolimus to either extended-release (ER)-tacrolimus or LifeCyclePharma (LCP)-tacrolimus. In this randomized, prospective, open-label, cross-over trial, adult kidney transplant recipients on a stable immunosuppressive regimen, including IR-tacrolimus, were randomized for conversion to ER-tacrolimus or LCP-tacrolimus, and for the order in which IR-tacrolimus and the once-daily formulations were taken. Patients were followed 6 months for each formulation, with monthly tacrolimus predose concentration assessments to calculate the IPV. The IPV was defined as the coefficient of variation (%) of dose corrected predose concentrations. Ninety-two patients were included for analysis of the primary outcome. No significant differences between the IPV of IR-tacrolimus (16.6%) and the combined once-daily formulations (18.3%) were observed (% difference +1.7%, 95% confidence interval [CI] -1.1% to -4.5%, p = 0.24). The IPV of LCP-tacrolimus (20.1%) was not significantly different from the IPV of ER-tacrolimus (16.5%, % difference +3.6%, 95% CI -0.1% to 7.3%, p = 0.06). In conclusion, the IPV did not decrease after switching from IR-tacrolimus to either ER-tacrolimus or LCP-tacrolimus. These results provide no arguments to switch kidney transplant recipients from twice-daily (IR) tacrolimus formulations to once-daily (modified-release) tacrolimus formulations when the aim is to lower the IPV.</p>","PeriodicalId":501617,"journal":{"name":"Clinical and Translational Science","volume":" ","pages":"930-941"},"PeriodicalIF":0.0000,"publicationDate":"2022-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/fd/ae/CTS-15-930.PMC9010272.pdf","citationCount":"5","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical and Translational Science","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1111/cts.13206","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/12/15 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 5
Abstract
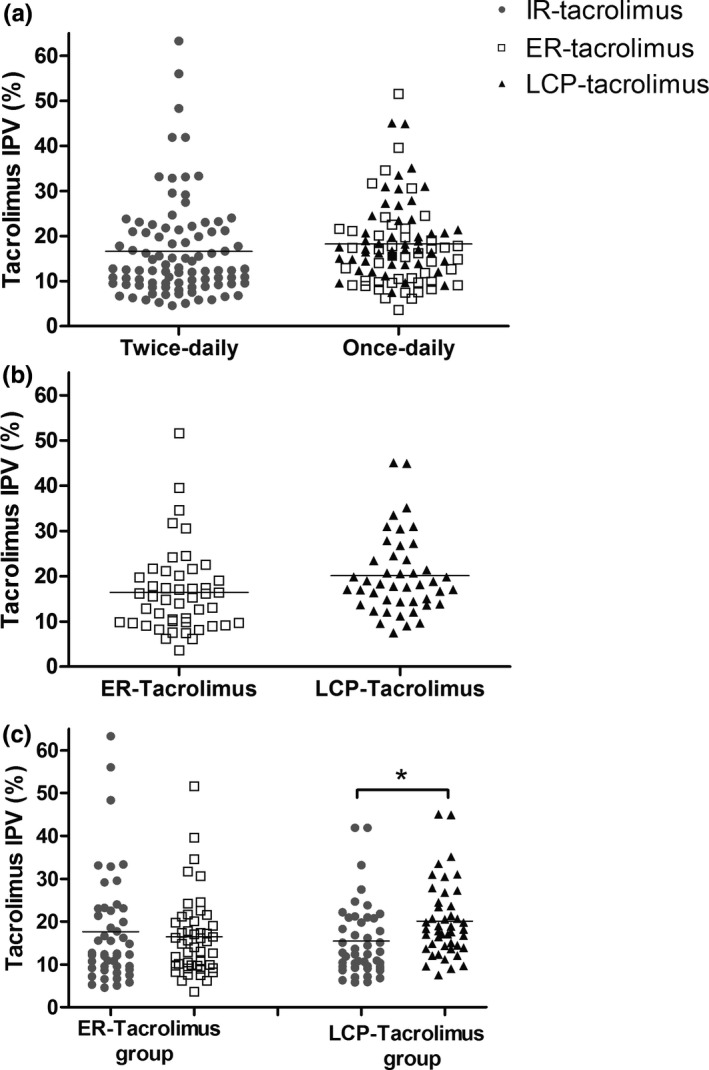
A high intrapatient variability (IPV) in tacrolimus exposure is a risk factor for poor long-term outcomes after kidney transplantation. The main objective of this trial was to investigate whether tacrolimus IPV decreases after switching patients from immediate-release (IR)-tacrolimus to either extended-release (ER)-tacrolimus or LifeCyclePharma (LCP)-tacrolimus. In this randomized, prospective, open-label, cross-over trial, adult kidney transplant recipients on a stable immunosuppressive regimen, including IR-tacrolimus, were randomized for conversion to ER-tacrolimus or LCP-tacrolimus, and for the order in which IR-tacrolimus and the once-daily formulations were taken. Patients were followed 6 months for each formulation, with monthly tacrolimus predose concentration assessments to calculate the IPV. The IPV was defined as the coefficient of variation (%) of dose corrected predose concentrations. Ninety-two patients were included for analysis of the primary outcome. No significant differences between the IPV of IR-tacrolimus (16.6%) and the combined once-daily formulations (18.3%) were observed (% difference +1.7%, 95% confidence interval [CI] -1.1% to -4.5%, p = 0.24). The IPV of LCP-tacrolimus (20.1%) was not significantly different from the IPV of ER-tacrolimus (16.5%, % difference +3.6%, 95% CI -0.1% to 7.3%, p = 0.06). In conclusion, the IPV did not decrease after switching from IR-tacrolimus to either ER-tacrolimus or LCP-tacrolimus. These results provide no arguments to switch kidney transplant recipients from twice-daily (IR) tacrolimus formulations to once-daily (modified-release) tacrolimus formulations when the aim is to lower the IPV.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


