Shakti Shrestha, Arjun Poudel, Magnolia Cardona, Kathryn J Steadman, Lisa M Nissen
{"title":"Impact of deprescribing dual-purpose medications on patient-related outcomes for older adults near end-of-life: a systematic review and meta-analysis.","authors":"Shakti Shrestha, Arjun Poudel, Magnolia Cardona, Kathryn J Steadman, Lisa M Nissen","doi":"10.1177/20420986211052343","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The decision to deprescribe medications used for both disease prevention and symptom control (dual-purpose medications or DPMs) is often challenging for clinicians. We aim to establish the impact of deprescribing DPMs on patient-related outcomes for older adults near end-of-life (EOL).</p><p><strong>Methods: </strong>This systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline. Literature was searched on PubMed, EMBASE, CINAHL, PsycINFO and Google Scholar until December 2019 for studies on deprescribing intervention with a control group (with or without randomisation); targeting ⩾65-year olds, at EOL, with at least one life-limiting illness and at least one potentially inappropriate DPM. We were interested in any patient-related outcomes. Studies with similar outcome assessment criteria were subjected to meta-analysis and narrative synthesis otherwise. The risk of bias was assessed using Cochrane Risk of Bias and ROBINS-I tools for randomised controlled trials (RCTs) and quasi-experimental non-randomised controlled studies, respectively.</p><p><strong>Results: </strong>Five studies covering 689 participants with mean age 81.6-85.7 years, the majority (74.6-100%) with dementia were included. The risk of bias was moderate to low. The deprescribing of DPMs lowered the risk of mortality (risk ratio (RR) = 0.59, 95% confidence interval (CI) = 0.44-0.79) and referral to acute care facilities (RR = 0.40, 95% CI = 0.22-0.73), but did not have a significant impact on the risk of falls, non-vertebral fracture, emergency presentation, unplanned hospital admission, or general practitioner visits. No significant difference was observed in the quality of life, physical and cognitive functions between the intervention and control groups.</p><p><strong>Conclusion: </strong>There is some evidence that deprescribing of DPMs for older adults near the EOL can lower the risk of mortality and referral to acute care facilities, but there are insufficient good-quality studies powered to confirm a benefit in terms of quality of life, physical or cognitive function, health service utilisation and adverse events.</p><p><strong>Plain language summary: </strong><b>What is the health impact of withdrawal or dose reduction of medication used for disease prevention and symptom control in older adults near end-of-life?</b> <b>Introduction:</b> Older adults (aged ⩾ 65 years) with advanced diseases such as cancer, dementia, and organ failure tend to have a limited life expectancy. With the progression of these diseases towards the end-of-life, the intensity for day-to-day supportive care becomes increasingly necessary. The use of medications for symptom management is a critical part of such care, but the use of medications for long-term disease prevention can become irrelevant due to the already shortened life expectancy and may become harmful due to alterations in physiology and pharmacology associated with age and frailty. This necessitates the withdrawal or dose reduction of inappropriate medications, the process called deprescribing. The decision to deprescribe medications used for both disease prevention and symptom control (DPMs) in this population is often challenging for clinicians. In this context, whether deprescribing of DPMs can improve patient-related health outcomes is unknown.<b>Methods:</b> Evidence from the literature was reviewed and analysed, and the quality of studies was assessed. Five studies were identified, which had 689 participants with an average age above 80 years and mostly suffering from dementia.<b>Results:</b> The analysis of these studies showed deprescribing of DPMs lowered the risk of death and referral to acute care facilities at 12 months but had no significant impact on falls, non-vertebral fractures, emergency presentations, unplanned hospital admission, general practitioner visits, quality of life, physical and mental functions.<b>Conclusion:</b> In conclusion, there were insufficient numbers of high-quality studies powered to confirm whether deprescribing of DPMs reduces adverse events, health service use, or improves the quality of life or functioning in older adults near the end of life.</p>","PeriodicalId":23012,"journal":{"name":"Therapeutic Advances in Drug Safety","volume":"12 ","pages":"20420986211052343"},"PeriodicalIF":3.4000,"publicationDate":"2021-10-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/8b/df/10.1177_20420986211052343.PMC8543710.pdf","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420986211052343","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 8
Abstract
Introduction: The decision to deprescribe medications used for both disease prevention and symptom control (dual-purpose medications or DPMs) is often challenging for clinicians. We aim to establish the impact of deprescribing DPMs on patient-related outcomes for older adults near end-of-life (EOL).
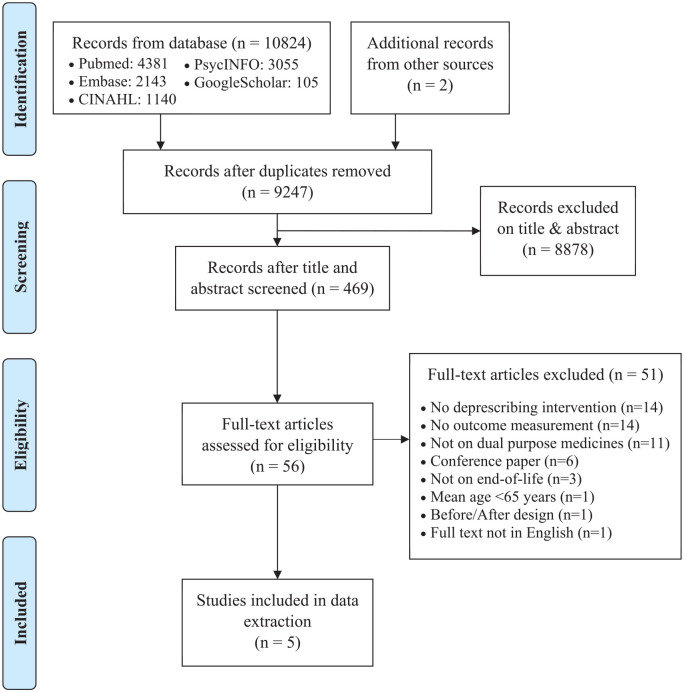
Methods: This systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guideline. Literature was searched on PubMed, EMBASE, CINAHL, PsycINFO and Google Scholar until December 2019 for studies on deprescribing intervention with a control group (with or without randomisation); targeting ⩾65-year olds, at EOL, with at least one life-limiting illness and at least one potentially inappropriate DPM. We were interested in any patient-related outcomes. Studies with similar outcome assessment criteria were subjected to meta-analysis and narrative synthesis otherwise. The risk of bias was assessed using Cochrane Risk of Bias and ROBINS-I tools for randomised controlled trials (RCTs) and quasi-experimental non-randomised controlled studies, respectively.
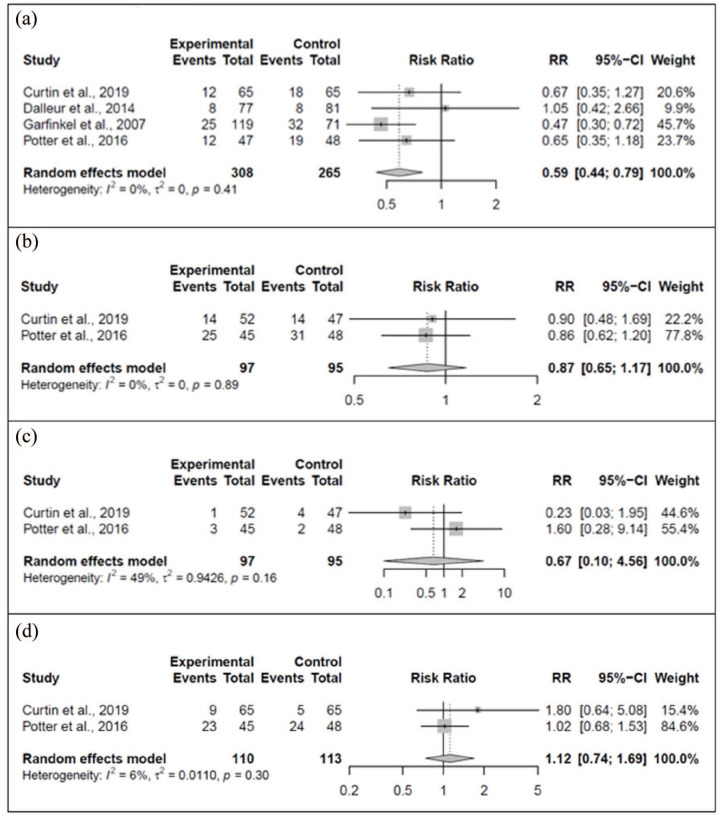
Results: Five studies covering 689 participants with mean age 81.6-85.7 years, the majority (74.6-100%) with dementia were included. The risk of bias was moderate to low. The deprescribing of DPMs lowered the risk of mortality (risk ratio (RR) = 0.59, 95% confidence interval (CI) = 0.44-0.79) and referral to acute care facilities (RR = 0.40, 95% CI = 0.22-0.73), but did not have a significant impact on the risk of falls, non-vertebral fracture, emergency presentation, unplanned hospital admission, or general practitioner visits. No significant difference was observed in the quality of life, physical and cognitive functions between the intervention and control groups.
Conclusion: There is some evidence that deprescribing of DPMs for older adults near the EOL can lower the risk of mortality and referral to acute care facilities, but there are insufficient good-quality studies powered to confirm a benefit in terms of quality of life, physical or cognitive function, health service utilisation and adverse events.
Plain language summary: What is the health impact of withdrawal or dose reduction of medication used for disease prevention and symptom control in older adults near end-of-life?Introduction: Older adults (aged ⩾ 65 years) with advanced diseases such as cancer, dementia, and organ failure tend to have a limited life expectancy. With the progression of these diseases towards the end-of-life, the intensity for day-to-day supportive care becomes increasingly necessary. The use of medications for symptom management is a critical part of such care, but the use of medications for long-term disease prevention can become irrelevant due to the already shortened life expectancy and may become harmful due to alterations in physiology and pharmacology associated with age and frailty. This necessitates the withdrawal or dose reduction of inappropriate medications, the process called deprescribing. The decision to deprescribe medications used for both disease prevention and symptom control (DPMs) in this population is often challenging for clinicians. In this context, whether deprescribing of DPMs can improve patient-related health outcomes is unknown.Methods: Evidence from the literature was reviewed and analysed, and the quality of studies was assessed. Five studies were identified, which had 689 participants with an average age above 80 years and mostly suffering from dementia.Results: The analysis of these studies showed deprescribing of DPMs lowered the risk of death and referral to acute care facilities at 12 months but had no significant impact on falls, non-vertebral fractures, emergency presentations, unplanned hospital admission, general practitioner visits, quality of life, physical and mental functions.Conclusion: In conclusion, there were insufficient numbers of high-quality studies powered to confirm whether deprescribing of DPMs reduces adverse events, health service use, or improves the quality of life or functioning in older adults near the end of life.
期刊介绍:
Therapeutic Advances in Drug Safety delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies pertaining to the safe use of drugs in patients.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in drug safety, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest on research across all areas of drug safety, including therapeutic drug monitoring, pharmacoepidemiology, adverse drug reactions, drug interactions, pharmacokinetics, pharmacovigilance, medication/prescribing errors, risk management, ethics and regulation.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


