Early toxicities of ultrahypofractionated stereotactic body radiotherapy for intermediate risk localized prostate cancer using cone-beam computed tomography and real-time three-dimensional transperineal ultrasound monitoring.
Eric Ka-Chai Lee, Ronnie Wing-Kin Leung, Hollis Siu-Leung Luk, Barry Bar-Wai Wo
{"title":"Early toxicities of ultrahypofractionated stereotactic body radiotherapy for intermediate risk localized prostate cancer using cone-beam computed tomography and real-time three-dimensional transperineal ultrasound monitoring.","authors":"Eric Ka-Chai Lee, Ronnie Wing-Kin Leung, Hollis Siu-Leung Luk, Barry Bar-Wai Wo","doi":"10.3857/roj.2020.00969","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>Image-guided radiotherapy (IGRT) is central to the safe and effective delivery of ultrahypofractionated (UF) stereotactic body radiotherapy (SBRT) for localized prostate cancer. However, the optimal IGRT modality remains uncertain. We aim to study the safety of performing UF-SBRT using cone-beam computed tomography (CBCT) and real-time transperineal ultrasound (TPUS) monitoring.</p><p><strong>Materials and methods: </strong>We retrospectively review the medical records of 26 patients who had received UF-SBRT for intermediate risk localized prostate cancer in our institution from October 2018 to December 2020. All patients were treated with SBRT without fiducial marker and received 35-40 Gy to the clinical target volume in 5 fractions over 2-5 weeks. CBCT was used to correct for interfraction displacement while intrafraction displacement of the prostate gland was monitored using Elekta Clarity Autoscan TPUS with 4 mm isotropic warning level. All patients also received neoadjuvant and concurrent androgen deprivation therapy for a total of 6 months. The primary endpoints were incidence of acute toxicities and patient reported urinary toxicities in terms of the International Prostate Symptom Score: before (IPSS1), at the completion of (IPSS2), and at 3-6 months (IPSS3) after SBRT.</p><p><strong>Results: </strong>All men were treated and followed up for at least 3 months after SBRT. Patients experienced transient worsening of their urinary symptoms at the end of SBRT but they usually recovered in 3-6 months afterwards. The median IPSS1, IPSS2, and IPSS3 were 12, 12.5, and 8, respectively. One patient developed grade 3 rectal bleeding which was related to underlying hemorrhoid. No other grade 3-4 acute toxicity was observed.</p><p><strong>Conclusion: </strong>It appears safe to deliver UF-SBRT without fiducial marker for prostate cancer patients using CBCT and non-invasive hybrid imaging modalities for positioning and tracking. Longer follow-up is necessary to monitor the treatment efficacy and long-term toxicities.</p>","PeriodicalId":46572,"journal":{"name":"Radiation Oncology Journal","volume":"39 3","pages":"239-245"},"PeriodicalIF":2.2000,"publicationDate":"2021-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/f0/e5/roj-2020-00969.PMC8497869.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation Oncology Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2020.00969","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/9/28 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
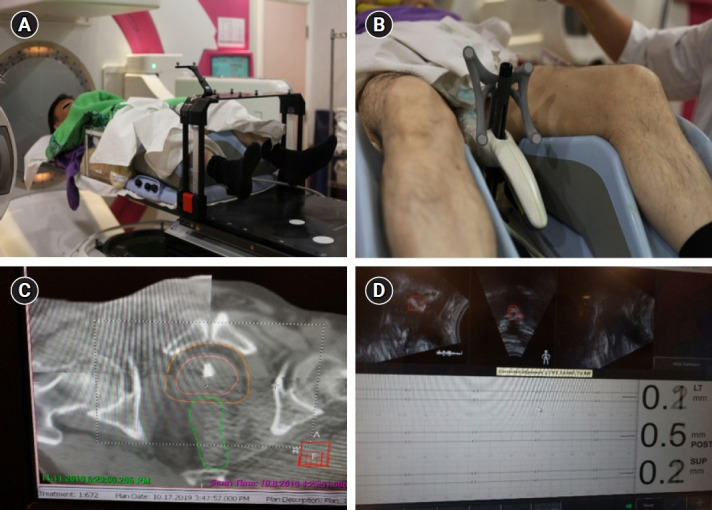
Purpose: Image-guided radiotherapy (IGRT) is central to the safe and effective delivery of ultrahypofractionated (UF) stereotactic body radiotherapy (SBRT) for localized prostate cancer. However, the optimal IGRT modality remains uncertain. We aim to study the safety of performing UF-SBRT using cone-beam computed tomography (CBCT) and real-time transperineal ultrasound (TPUS) monitoring.
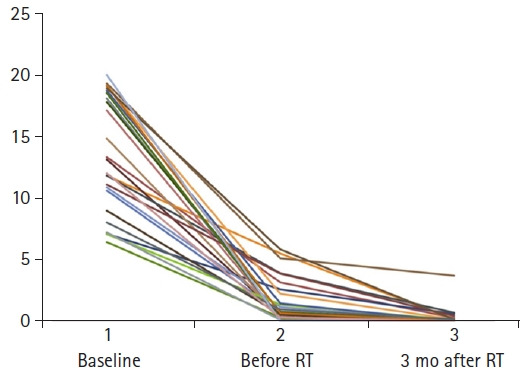
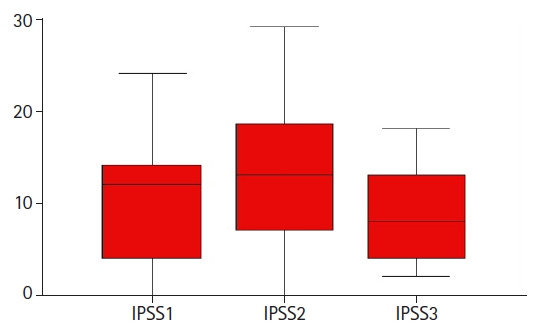
Materials and methods: We retrospectively review the medical records of 26 patients who had received UF-SBRT for intermediate risk localized prostate cancer in our institution from October 2018 to December 2020. All patients were treated with SBRT without fiducial marker and received 35-40 Gy to the clinical target volume in 5 fractions over 2-5 weeks. CBCT was used to correct for interfraction displacement while intrafraction displacement of the prostate gland was monitored using Elekta Clarity Autoscan TPUS with 4 mm isotropic warning level. All patients also received neoadjuvant and concurrent androgen deprivation therapy for a total of 6 months. The primary endpoints were incidence of acute toxicities and patient reported urinary toxicities in terms of the International Prostate Symptom Score: before (IPSS1), at the completion of (IPSS2), and at 3-6 months (IPSS3) after SBRT.
Results: All men were treated and followed up for at least 3 months after SBRT. Patients experienced transient worsening of their urinary symptoms at the end of SBRT but they usually recovered in 3-6 months afterwards. The median IPSS1, IPSS2, and IPSS3 were 12, 12.5, and 8, respectively. One patient developed grade 3 rectal bleeding which was related to underlying hemorrhoid. No other grade 3-4 acute toxicity was observed.
Conclusion: It appears safe to deliver UF-SBRT without fiducial marker for prostate cancer patients using CBCT and non-invasive hybrid imaging modalities for positioning and tracking. Longer follow-up is necessary to monitor the treatment efficacy and long-term toxicities.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


