Sustaining a Multidisciplinary, Single-Institution, Postoperative Mobilization Clinical Practice Improvement Program Following Hepatopancreatobiliary Surgery During the COVID-19 Pandemic: Prospective Cohort Study.
Kai Siang Chan, Bei Wang, Yen Pin Tan, Jaclyn Jie Ling Chow, Ee Ling Ong, Sameer P Junnarkar, Jee Keem Low, Cheong Wei Terence Huey, Vishal G Shelat
{"title":"Sustaining a Multidisciplinary, Single-Institution, Postoperative Mobilization Clinical Practice Improvement Program Following Hepatopancreatobiliary Surgery During the COVID-19 Pandemic: Prospective Cohort Study.","authors":"Kai Siang Chan, Bei Wang, Yen Pin Tan, Jaclyn Jie Ling Chow, Ee Ling Ong, Sameer P Junnarkar, Jee Keem Low, Cheong Wei Terence Huey, Vishal G Shelat","doi":"10.2196/30473","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Enhanced Recovery After Surgery (ERAS) protocol has been recently extended to hepatopancreatobiliary (HPB) surgery, with excellent outcomes reported. Early mobilization is an essential facet of the ERAS protocol, but compliance has been reported to be poor. We recently reported our success in a 6-month clinical practice improvement program (CPIP) for early postoperative mobilization. During the COVID-19 pandemic, we experienced reduced staffing and resource availability, which can make CPIP sustainability difficult.</p><p><strong>Objective: </strong>We report outcomes at 1 year following the implementation of our CPIP to improve postoperative mobilization in patients undergoing major HPB surgery during the COVID-19 pandemic.</p><p><strong>Methods: </strong>We divided our study into 4 phases-phase 1: before CPIP implementation (January to April 2019); phase 2: CPIP implementation (May to September 2019); phase 3: post-CPIP implementation but prior to the COVID-19 pandemic (October 2019 to March 2020); and phase 4: post-CPIP implementation and during the pandemic (April 2020 to September 2020). Major HPB surgery was defined as any surgery on the liver, pancreas, and biliary system with a duration of >2 hours and with an anticipated blood loss of ≥500 ml. Study variables included length of hospital stay, distance ambulated on postoperative day (POD) 2, morbidity, balance measures (incidence of fall and accidental dislodgement of drains), and reasons for failure to achieve targets. Successful mobilization was defined as the ability to sit out of bed for >6 hours on POD 1 and ambulate ≥30 m on POD 2. The target mobilization rate was ≥75%.</p><p><strong>Results: </strong>A total of 114 patients underwent major HPB surgery from phases 2 to 4 of our study, with 33 (29.0%), 45 (39.5%), and 36 (31.6%) patients in phases 2, 3, and 4, respectively. No baseline patient demographic data were collected for phase 1 (pre-CPIP implementation). The majority of the patients were male (n=79, 69.3%) and underwent hepatic surgery (n=92, 80.7%). A total of 76 (66.7%) patients underwent ON-Q PainBuster insertion intraoperatively. The median mobilization rate was 22% for phase 1, 78% for phases 2 and 3 combined, and 79% for phase 4. The mean pain score was 2.7 (SD 1.0) on POD 1 and 1.8 (SD 1.5) on POD 2. The median length of hospitalization was 6 days (IQR 5-11.8). There were no falls or accidental dislodgement of drains. Six patients (5.3%) had pneumonia, and 21 (18.4%) patients failed to ambulate ≥30 m on POD 2 from phases 2 to 4. The most common reason for failure to achieve the ambulation target was pain (6/21, 28.6%) and lethargy or giddiness (5/21, 23.8%).</p><p><strong>Conclusions: </strong>This follow-up study demonstrates the sustainability of our CPIP in improving early postoperative mobilization rates following major HPB surgery 1 year after implementation, even during the COVID-19 pandemic. Further large-scale, multi-institutional prospective studies should be conducted to assess compliance and determine its sustainability.</p>","PeriodicalId":73557,"journal":{"name":"JMIR perioperative medicine","volume":"4 2","pages":"e30473"},"PeriodicalIF":0.0000,"publicationDate":"2021-10-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8496752/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JMIR perioperative medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2196/30473","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: The Enhanced Recovery After Surgery (ERAS) protocol has been recently extended to hepatopancreatobiliary (HPB) surgery, with excellent outcomes reported. Early mobilization is an essential facet of the ERAS protocol, but compliance has been reported to be poor. We recently reported our success in a 6-month clinical practice improvement program (CPIP) for early postoperative mobilization. During the COVID-19 pandemic, we experienced reduced staffing and resource availability, which can make CPIP sustainability difficult.
Objective: We report outcomes at 1 year following the implementation of our CPIP to improve postoperative mobilization in patients undergoing major HPB surgery during the COVID-19 pandemic.
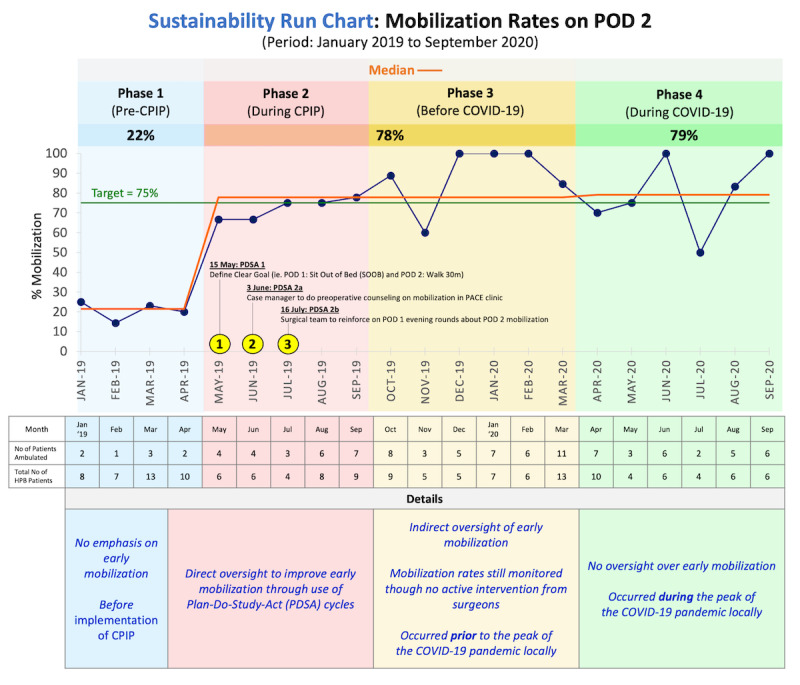
Methods: We divided our study into 4 phases-phase 1: before CPIP implementation (January to April 2019); phase 2: CPIP implementation (May to September 2019); phase 3: post-CPIP implementation but prior to the COVID-19 pandemic (October 2019 to March 2020); and phase 4: post-CPIP implementation and during the pandemic (April 2020 to September 2020). Major HPB surgery was defined as any surgery on the liver, pancreas, and biliary system with a duration of >2 hours and with an anticipated blood loss of ≥500 ml. Study variables included length of hospital stay, distance ambulated on postoperative day (POD) 2, morbidity, balance measures (incidence of fall and accidental dislodgement of drains), and reasons for failure to achieve targets. Successful mobilization was defined as the ability to sit out of bed for >6 hours on POD 1 and ambulate ≥30 m on POD 2. The target mobilization rate was ≥75%.
Results: A total of 114 patients underwent major HPB surgery from phases 2 to 4 of our study, with 33 (29.0%), 45 (39.5%), and 36 (31.6%) patients in phases 2, 3, and 4, respectively. No baseline patient demographic data were collected for phase 1 (pre-CPIP implementation). The majority of the patients were male (n=79, 69.3%) and underwent hepatic surgery (n=92, 80.7%). A total of 76 (66.7%) patients underwent ON-Q PainBuster insertion intraoperatively. The median mobilization rate was 22% for phase 1, 78% for phases 2 and 3 combined, and 79% for phase 4. The mean pain score was 2.7 (SD 1.0) on POD 1 and 1.8 (SD 1.5) on POD 2. The median length of hospitalization was 6 days (IQR 5-11.8). There were no falls or accidental dislodgement of drains. Six patients (5.3%) had pneumonia, and 21 (18.4%) patients failed to ambulate ≥30 m on POD 2 from phases 2 to 4. The most common reason for failure to achieve the ambulation target was pain (6/21, 28.6%) and lethargy or giddiness (5/21, 23.8%).
Conclusions: This follow-up study demonstrates the sustainability of our CPIP in improving early postoperative mobilization rates following major HPB surgery 1 year after implementation, even during the COVID-19 pandemic. Further large-scale, multi-institutional prospective studies should be conducted to assess compliance and determine its sustainability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


