Organizational contextual factors that predict success of a quality improvement collaborative approach to enhance integrated HIV-tuberculosis services: a sub-study of the Scaling up TB/HIV Integration trial.
Santhanalakshmi Gengiah, Catherine Connolly, Nonhlanhla Yende-Zuma, Pierre M Barker, Andrew J Nunn, Nesri Padayatchi, Myra Taylor, Marian Loveday, Kogieleum Naidoo
{"title":"Organizational contextual factors that predict success of a quality improvement collaborative approach to enhance integrated HIV-tuberculosis services: a sub-study of the Scaling up TB/HIV Integration trial.","authors":"Santhanalakshmi Gengiah, Catherine Connolly, Nonhlanhla Yende-Zuma, Pierre M Barker, Andrew J Nunn, Nesri Padayatchi, Myra Taylor, Marian Loveday, Kogieleum Naidoo","doi":"10.1186/s13012-021-01155-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A quality improvement (QI) collaborative approach to enhancing integrated HIV-Tuberculosis (TB) services may be effective in scaling up and improving the quality of service delivery. Little is known of the role of organizational contextual factors (OCFs) in influencing the success of QI collaboratives. This study aims to determine which OCFs were associated with improvement in a QI collaborative intervention to enhance integrated HIV-TB services delivery.</p><p><strong>Methods: </strong>This is a nested sub-study embedded in a cluster-randomized controlled trial. Sixteen nurse supervisors (clusters) overseeing 40 clinics were randomized (1:1) to receive QI training and mentorship, or standard of care support (SOC). In the QI arm, eight nurse supervisors and 20 clinics formed a \"collaborative\" which aimed to improve HIV-TB process indicators, namely HIV testing, TB screening, isoniazid preventive therapy (IPT) initiations, viral load testing, and antiretroviral therapy for TB patients. OCFs measured at baseline were physical infrastructure, key staff, flexibility of clinic hours, monitoring data for improvement (MDI), and leadership support. Surveys were administered to clinic staff at baseline and month 12 to assess perceptions of supportiveness of contexts for change, and clinic organization for delivering integrated HIV-TB services. Linear mixed modelling was used to test for associations between OCFs and HIV-TB process indicators.</p><p><strong>Results: </strong>A total of 209 clinic staff participated in the study; 97 (46.4%) and 112 (53.6%) from QI and SOC arms, respectively. There were no differences between the QI and SOC arms scores achieved for physical infrastructure (78.9% vs 64.7%; p = 0.058), key staff (95.8 vs 92; p = 0.270), clinic hours (66.9 vs 65.5; p = 0.900), MDI (63.3 vs 65; p = 0.875, leadership support (46.0 vs 57.4; p = 0.265), and perceptions of supportiveness of contexts for change (76.2 vs 79.7; p = 0.128 and clinic organization for delivering integrated HIV-TB services (74.1 vs 80.1; p = 0.916). IPT initiation was the only indicator that was significantly improved in the parent study. MDI was a significantly associated with increasing IPT initiation rates [beta coefficient (β) = 0.004; p = 0.004].</p><p><strong>Discussion: </strong>MDI is a practice that should be fostered in public health facilities to increase the likelihood of success of future QI collaboratives to improve HIV-TB service delivery.</p><p><strong>Trial registration: </strong>Clinicaltrials.gov , NCT02654613 . Registered 01 June 2015.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"88"},"PeriodicalIF":0.0000,"publicationDate":"2021-09-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8447673/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s13012-021-01155-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A quality improvement (QI) collaborative approach to enhancing integrated HIV-Tuberculosis (TB) services may be effective in scaling up and improving the quality of service delivery. Little is known of the role of organizational contextual factors (OCFs) in influencing the success of QI collaboratives. This study aims to determine which OCFs were associated with improvement in a QI collaborative intervention to enhance integrated HIV-TB services delivery.
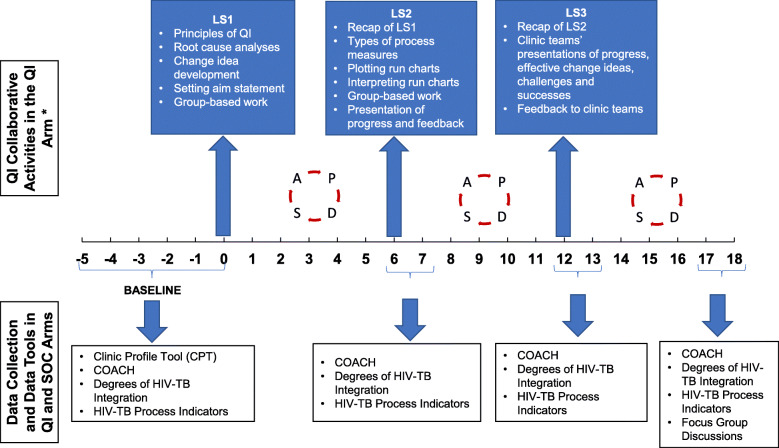
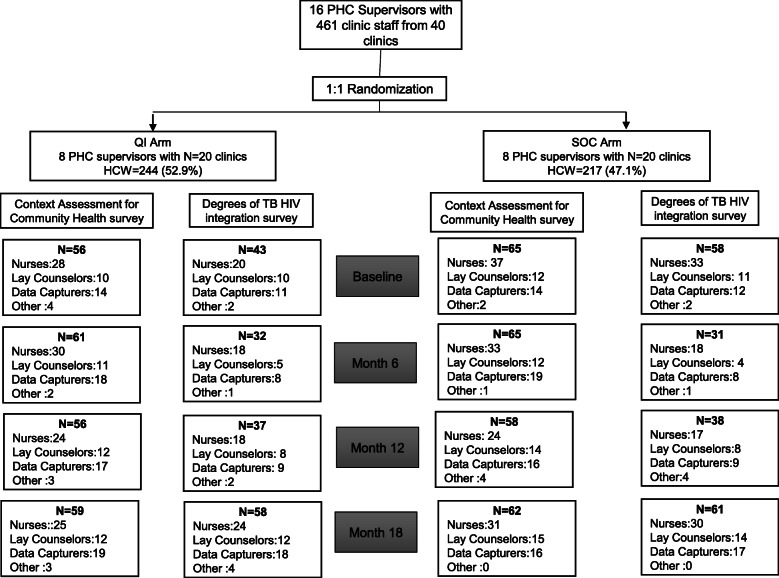
Methods: This is a nested sub-study embedded in a cluster-randomized controlled trial. Sixteen nurse supervisors (clusters) overseeing 40 clinics were randomized (1:1) to receive QI training and mentorship, or standard of care support (SOC). In the QI arm, eight nurse supervisors and 20 clinics formed a "collaborative" which aimed to improve HIV-TB process indicators, namely HIV testing, TB screening, isoniazid preventive therapy (IPT) initiations, viral load testing, and antiretroviral therapy for TB patients. OCFs measured at baseline were physical infrastructure, key staff, flexibility of clinic hours, monitoring data for improvement (MDI), and leadership support. Surveys were administered to clinic staff at baseline and month 12 to assess perceptions of supportiveness of contexts for change, and clinic organization for delivering integrated HIV-TB services. Linear mixed modelling was used to test for associations between OCFs and HIV-TB process indicators.
Results: A total of 209 clinic staff participated in the study; 97 (46.4%) and 112 (53.6%) from QI and SOC arms, respectively. There were no differences between the QI and SOC arms scores achieved for physical infrastructure (78.9% vs 64.7%; p = 0.058), key staff (95.8 vs 92; p = 0.270), clinic hours (66.9 vs 65.5; p = 0.900), MDI (63.3 vs 65; p = 0.875, leadership support (46.0 vs 57.4; p = 0.265), and perceptions of supportiveness of contexts for change (76.2 vs 79.7; p = 0.128 and clinic organization for delivering integrated HIV-TB services (74.1 vs 80.1; p = 0.916). IPT initiation was the only indicator that was significantly improved in the parent study. MDI was a significantly associated with increasing IPT initiation rates [beta coefficient (β) = 0.004; p = 0.004].
Discussion: MDI is a practice that should be fostered in public health facilities to increase the likelihood of success of future QI collaboratives to improve HIV-TB service delivery.
Trial registration: Clinicaltrials.gov , NCT02654613 . Registered 01 June 2015.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


