Jintanat Ananworanich, Robin Mogg, Michael W Dunne, Mohamed Bassyouni, Consuela Vera David, Erika Gonzalez, Taryn Rogalski-Salter, Heather Shih, Jared Silverman, Jeroen Medema, Penny Heaton
{"title":"Randomized Study of Rivaroxaban vs Placebo on Disease Progression and Symptoms Resolution in High-Risk Adults With Mild Coronavirus Disease 2019.","authors":"Jintanat Ananworanich, Robin Mogg, Michael W Dunne, Mohamed Bassyouni, Consuela Vera David, Erika Gonzalez, Taryn Rogalski-Salter, Heather Shih, Jared Silverman, Jeroen Medema, Penny Heaton","doi":"10.1093/cid/ciab813","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Severe acute respiratory syndrome coronavirus 2 infection may be associated with a prothrombotic state, predisposing patients for a progressive disease course. We investigated whether rivaroxaban, a direct oral anticoagulant factor Xa inhibitor, would reduce coronavirus disease 2019 (COVID-19) progression.</p><p><strong>Methods: </strong>Adults (N = 497) with mild COVID-19 symptoms and at high risk for COVID-19 progression based on age, body mass index, or comorbidity were randomized 1:1 to either daily oral rivaroxaban 10 mg (N = 246) or placebo equivalent (N = 251) for 21 days and followed to day 35. Primary end points were safety and progression. Absolute difference in progression risk was assessed using a stratified Miettinen and Nurminen method.</p><p><strong>Results: </strong>The study was terminated after 497 of the target 600 participants were enrolled due to a prespecified interim analysis of the first 200 participants that crossed the futility boundary for the primary efficacy end point in the intent-to-treat population. Enrollees were 85% aged <65 years; 60% female; 27% Hispanic, Black, or other minorities; and 69% with ≥2 comorbidities. Rivaroxaban was well tolerated. Disease progression rates were 46 of 222 (20.7%) in rivaroxaban vs 44 of 222 (19.8%) in placebo groups, with a risk difference of -1.0 (95% confidence interval, -6.4 to 8.4; P = .78).</p><p><strong>Conclusions: </strong>We did not demonstrate an impact of rivaroxaban on disease progression in high-risk adults with mild COVID-19. There remains a critical public health gap in identifying scalable effective therapies for high-risk people in the outpatient setting to prevent COVID-19 progression.</p>","PeriodicalId":10421,"journal":{"name":"Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America","volume":" ","pages":"e473-e481"},"PeriodicalIF":0.0000,"publicationDate":"2022-08-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8522357/pdf/","citationCount":"22","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Infectious Diseases: An Official Publication of the Infectious Diseases Society of America","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/cid/ciab813","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 22
Abstract
Background: Severe acute respiratory syndrome coronavirus 2 infection may be associated with a prothrombotic state, predisposing patients for a progressive disease course. We investigated whether rivaroxaban, a direct oral anticoagulant factor Xa inhibitor, would reduce coronavirus disease 2019 (COVID-19) progression.
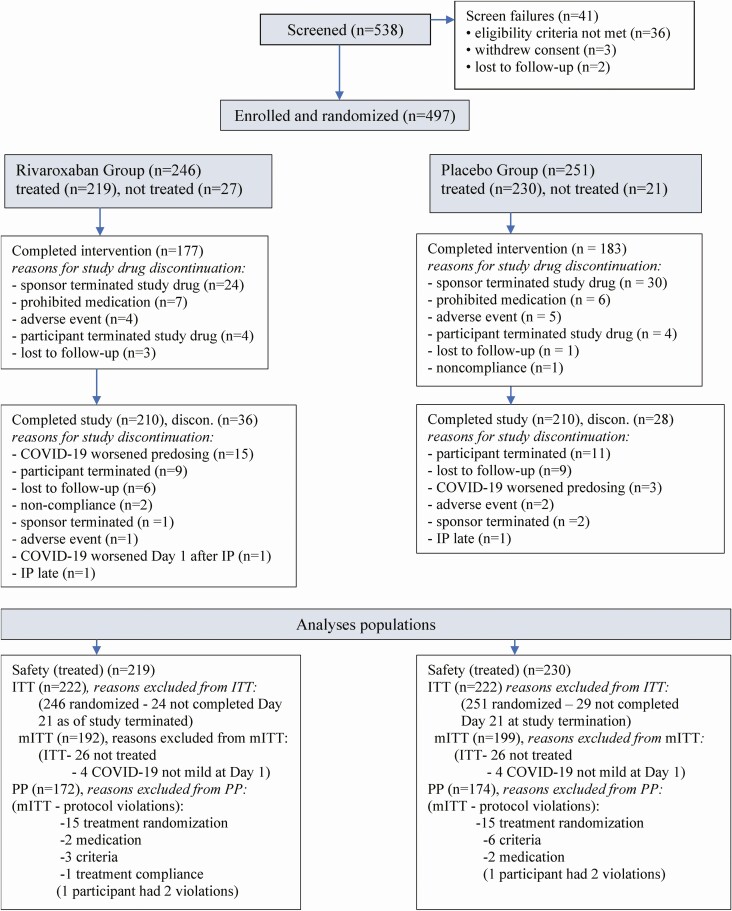
Methods: Adults (N = 497) with mild COVID-19 symptoms and at high risk for COVID-19 progression based on age, body mass index, or comorbidity were randomized 1:1 to either daily oral rivaroxaban 10 mg (N = 246) or placebo equivalent (N = 251) for 21 days and followed to day 35. Primary end points were safety and progression. Absolute difference in progression risk was assessed using a stratified Miettinen and Nurminen method.
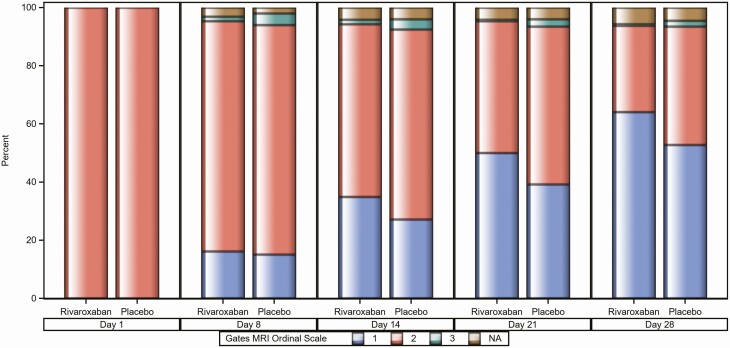
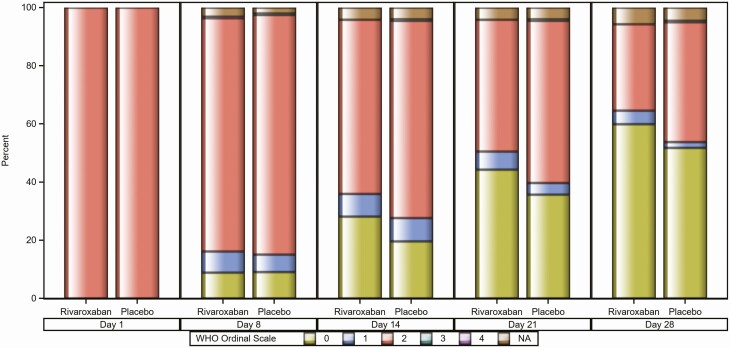
Results: The study was terminated after 497 of the target 600 participants were enrolled due to a prespecified interim analysis of the first 200 participants that crossed the futility boundary for the primary efficacy end point in the intent-to-treat population. Enrollees were 85% aged <65 years; 60% female; 27% Hispanic, Black, or other minorities; and 69% with ≥2 comorbidities. Rivaroxaban was well tolerated. Disease progression rates were 46 of 222 (20.7%) in rivaroxaban vs 44 of 222 (19.8%) in placebo groups, with a risk difference of -1.0 (95% confidence interval, -6.4 to 8.4; P = .78).
Conclusions: We did not demonstrate an impact of rivaroxaban on disease progression in high-risk adults with mild COVID-19. There remains a critical public health gap in identifying scalable effective therapies for high-risk people in the outpatient setting to prevent COVID-19 progression.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


