Marlot Johanna Blaak, Raad Fadaak, Jan M Davies, Nicole Pinto, John Conly, Myles Leslie
{"title":"Virtual tabletop simulations for primary care pandemic preparedness and response.","authors":"Marlot Johanna Blaak, Raad Fadaak, Jan M Davies, Nicole Pinto, John Conly, Myles Leslie","doi":"10.1136/bmjstel-2020-000854","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>The COVID-19 pandemic prompted widescale use of clinical simulations to improve procedures and practices. We outline our deployment of a virtual tabletop simulation (TTS) method in primary care (PC) clinics across Alberta, Canada. We summarise the quality and safety improvements from this method and report end users' perspectives on key elements.</p><p><strong>Methods: </strong>Our virtual TTS used teleconferencing software alongside digital whiteboards to walk clinic stakeholders through patient scenarios. Participants reviewed and rehearsed their workflows and care practices. The goal was for staff to take ownership over gaps and codesigned solutions. After simulation sessions, follow-up interviews were conducted to collect feedback.</p><p><strong>Results: </strong>These sessions helped PC staff identify and codesign solutions for clinical hazards and threats. These included the flow of patients through clinics, communications, redesignation of physical spaces, and adaptation of guidance for cleaning and personal protective equipment use. End users reported sessions provided neutral spaces to discuss practice changes and built confidence in delivering safe care during the pandemic.</p><p><strong>Discussion: </strong>TTS has not been extensively deployed to improve clinical practice in outpatient environments. We show how virtual TTS can bridge gaps between knowledge and practice by offering a guided space to rehearse clinical changes. We show that virtual TTS can be used in multiple contexts to help identify hazards, improve safety and build confidence in professional teams adapting to rapid changes in both policies and practices. While our sessions were conducted in Alberta, our results suggest this method may be deployed in other contexts, including low-resource settings.</p>","PeriodicalId":44757,"journal":{"name":"BMJ Simulation & Technology Enhanced Learning","volume":" ","pages":"487-493"},"PeriodicalIF":1.1000,"publicationDate":"2021-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1136/bmjstel-2020-000854","citationCount":"6","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Simulation & Technology Enhanced Learning","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjstel-2020-000854","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/4/13 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"Social Sciences","Score":null,"Total":0}
引用次数: 6
Abstract
Introduction: The COVID-19 pandemic prompted widescale use of clinical simulations to improve procedures and practices. We outline our deployment of a virtual tabletop simulation (TTS) method in primary care (PC) clinics across Alberta, Canada. We summarise the quality and safety improvements from this method and report end users' perspectives on key elements.
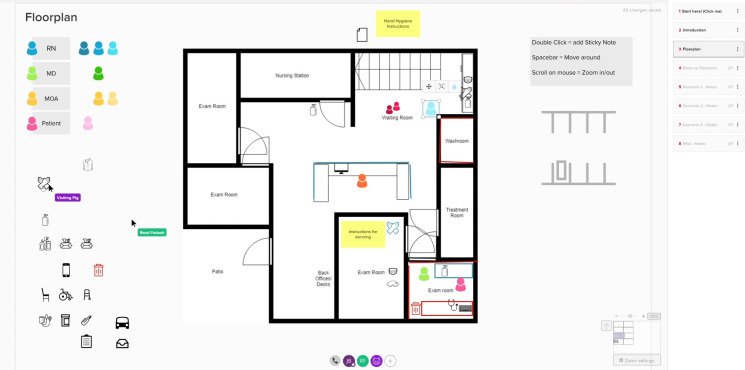
Methods: Our virtual TTS used teleconferencing software alongside digital whiteboards to walk clinic stakeholders through patient scenarios. Participants reviewed and rehearsed their workflows and care practices. The goal was for staff to take ownership over gaps and codesigned solutions. After simulation sessions, follow-up interviews were conducted to collect feedback.
Results: These sessions helped PC staff identify and codesign solutions for clinical hazards and threats. These included the flow of patients through clinics, communications, redesignation of physical spaces, and adaptation of guidance for cleaning and personal protective equipment use. End users reported sessions provided neutral spaces to discuss practice changes and built confidence in delivering safe care during the pandemic.
Discussion: TTS has not been extensively deployed to improve clinical practice in outpatient environments. We show how virtual TTS can bridge gaps between knowledge and practice by offering a guided space to rehearse clinical changes. We show that virtual TTS can be used in multiple contexts to help identify hazards, improve safety and build confidence in professional teams adapting to rapid changes in both policies and practices. While our sessions were conducted in Alberta, our results suggest this method may be deployed in other contexts, including low-resource settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



