Bone remodeling and implant migration of uncemented femoral and cemented asymmetrical tibial components in total knee arthroplasty - DXA and RSA evaluation with 2-year follow up.
Müjgan Yilmaz, Christina Enciso Holm, Thomas Lind, Gunnar Flivik, Anders Odgaard, Michael Mørk Petersen
{"title":"Bone remodeling and implant migration of uncemented femoral and cemented asymmetrical tibial components in total knee arthroplasty - DXA and RSA evaluation with 2-year follow up.","authors":"Müjgan Yilmaz, Christina Enciso Holm, Thomas Lind, Gunnar Flivik, Anders Odgaard, Michael Mørk Petersen","doi":"10.1186/s43019-021-00111-5","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Aseptic loosening is one of the major reasons for late revision in total knee arthroplasty (TKA). The risk of aseptic loosening can be detected using radiostereometric analysis (RSA), whereby micromovements (migration) can be measured, and thus RSA is recommended in the phased introduction of orthopedic implants. Decrease in bone mineral density (BMD), as measured by dual-energy x ray absorptiometry (DXA), is related to the breaking strength of the bone, which is measured concurrently by RSA. The aim of the study was to evaluate bone remodeling and implant migration with cemented asymmetrical tibial and uncemented femoral components after TKA with a follow up period of 2 years.</p><p><strong>Methods: </strong>This was a prospective longitudinal cohort study of 29 patients (number of female/male patients 17/12, mean age 65.2 years), received a hybrid Persona® TKA (Zimmer Biomet, Warsaw, IN, USA) consisting of a cemented tibial, an all-polyethylene patella, and uncemented trabecular metal femoral components. Follow up: preoperative, 1 week, and 3, 6, 12 and 24 months after surgery, and double examinations for RSA and DXA were performed at 12 months. RSA results were presented as maximal total point of motion (MTPM) and segmental motion (translation and rotation), and DXA results were presented as changes in BMD in different regions of interest (ROI).</p><p><strong>Results: </strong>MTPM at 3, 6, 12, and 24 months was 0.65 mm, 0.84 mm, 0.92 mm, and 0.96 mm for the femoral component and 0.54 mm, 0.60 mm, 0.64 mm, and 0.68 mm, respectively, for the tibial component. The highest MTPM occurred within the first 3 months. Afterwards most of the curves flattened and stabilized. Between 12 and 24 months after surgery, 16% of femoral components had migrated by more than 0.10 mm and 15% of tibial components had migrated by more than 0.2 mm. Percentage change in BMD in each ROI for distal femur was as follows: ROI I 26.7%, ROI II 9.2% and ROI III 3.3%. BMD and at the proximal tibia: ROI I 8.2%, ROI II 8.6% and ROI III 7.0% after 2 years compared with 1 week postoperative results. There was no significant correlation between maximal percentwise change in BMD and MTPM after 2 years.</p><p><strong>Conclusion: </strong>Migration patterns and changes in BMD related to femoral components after TKA in our study correspond well with previous studies; we observed marginally greater migration with the tibial component.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":"33 1","pages":"25"},"PeriodicalIF":4.4000,"publicationDate":"2021-08-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8369662/pdf/","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-021-00111-5","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Aseptic loosening is one of the major reasons for late revision in total knee arthroplasty (TKA). The risk of aseptic loosening can be detected using radiostereometric analysis (RSA), whereby micromovements (migration) can be measured, and thus RSA is recommended in the phased introduction of orthopedic implants. Decrease in bone mineral density (BMD), as measured by dual-energy x ray absorptiometry (DXA), is related to the breaking strength of the bone, which is measured concurrently by RSA. The aim of the study was to evaluate bone remodeling and implant migration with cemented asymmetrical tibial and uncemented femoral components after TKA with a follow up period of 2 years.
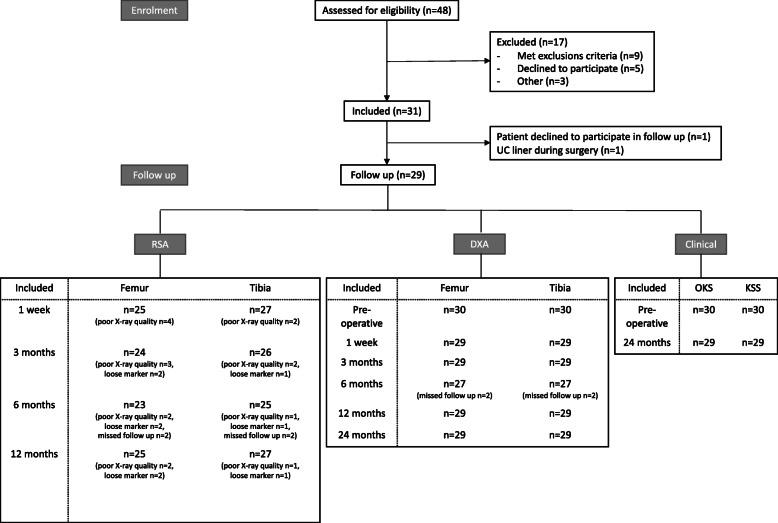
Methods: This was a prospective longitudinal cohort study of 29 patients (number of female/male patients 17/12, mean age 65.2 years), received a hybrid Persona® TKA (Zimmer Biomet, Warsaw, IN, USA) consisting of a cemented tibial, an all-polyethylene patella, and uncemented trabecular metal femoral components. Follow up: preoperative, 1 week, and 3, 6, 12 and 24 months after surgery, and double examinations for RSA and DXA were performed at 12 months. RSA results were presented as maximal total point of motion (MTPM) and segmental motion (translation and rotation), and DXA results were presented as changes in BMD in different regions of interest (ROI).
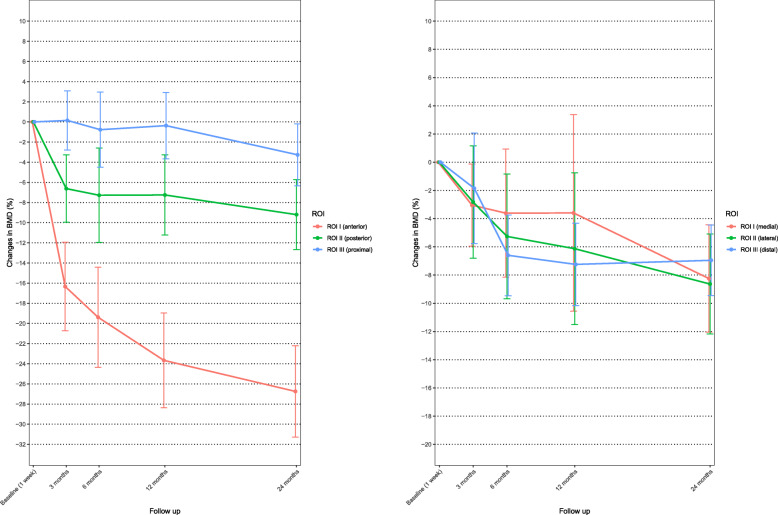
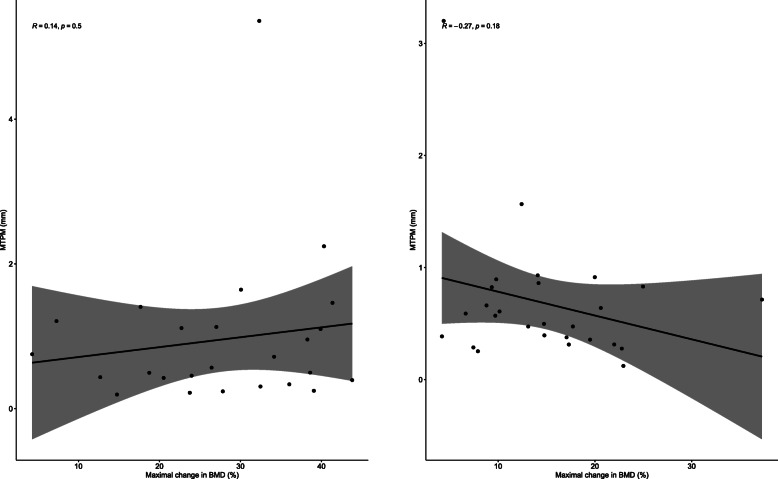
Results: MTPM at 3, 6, 12, and 24 months was 0.65 mm, 0.84 mm, 0.92 mm, and 0.96 mm for the femoral component and 0.54 mm, 0.60 mm, 0.64 mm, and 0.68 mm, respectively, for the tibial component. The highest MTPM occurred within the first 3 months. Afterwards most of the curves flattened and stabilized. Between 12 and 24 months after surgery, 16% of femoral components had migrated by more than 0.10 mm and 15% of tibial components had migrated by more than 0.2 mm. Percentage change in BMD in each ROI for distal femur was as follows: ROI I 26.7%, ROI II 9.2% and ROI III 3.3%. BMD and at the proximal tibia: ROI I 8.2%, ROI II 8.6% and ROI III 7.0% after 2 years compared with 1 week postoperative results. There was no significant correlation between maximal percentwise change in BMD and MTPM after 2 years.
Conclusion: Migration patterns and changes in BMD related to femoral components after TKA in our study correspond well with previous studies; we observed marginally greater migration with the tibial component.
背景:无菌性松动是全膝关节置换术(TKA)后期翻修的主要原因之一。无菌性松动的风险可以使用放射立体分析(RSA)来检测,由此可以测量微运动(迁移),因此推荐在分阶段引入骨科植入物时使用RSA。双能x射线吸收仪(DXA)测量的骨密度(BMD)的下降与骨的断裂强度有关,而骨的断裂强度是通过RSA同时测量的。本研究的目的是评估TKA术后骨重塑和不对称胫骨和非骨水泥股骨假体的植入物迁移,随访2年。方法:这是一项前瞻性纵向队列研究,29例患者(男女人数17/12,平均年龄65.2岁)接受混合Persona®TKA (Zimmer Biomet, Warsaw, IN, USA),由骨水泥胫骨、全聚乙烯髌骨和未骨水泥金属股骨小梁组成。随访:术前、术后1周、术后3、6、12、24个月,术后12个月行RSA、DXA双重检查。RSA结果显示为最大总运动点(MTPM)和节段运动(平移和旋转),DXA结果显示为不同感兴趣区域(ROI)的骨密度变化。结果:3、6、12和24个月时,股骨椎体的MTPM分别为0.65 mm、0.84 mm、0.92 mm和0.96 mm,胫骨椎体的MTPM分别为0.54 mm、0.60 mm、0.64 mm和0.68 mm。MTPM最高发生在前3个月内。之后,大部分曲线变平并趋于稳定。术后12 - 24个月,16%的股骨假体移位超过0.10 mm, 15%的胫骨假体移位超过0.2 mm。各ROI股骨远端骨密度变化百分比如下:ROI I 26.7%, ROI II 9.2%, ROI III 3.3%。骨密度和胫骨近端:与术后1周的结果相比,2年后ROI I为8.2%,ROI II为8.6%,ROI III为7.0%。2年后BMD的最大百分比变化与MTPM之间无显著相关性。结论:本研究中TKA术后股骨相关构件的迁移模式和骨密度变化与既往研究一致;我们观察到胫骨部分有较大的移位。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


