{"title":"Evaluation of drug-drug interactions in hospitalized patients on medications for OUD.","authors":"Olivia Berger, Katherine Rector, Jacqueline Meredith, Jamielynn Sebaaly","doi":"10.9740/mhc.2021.07.231","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Medications used to treat OUD have common metabolic pathways and pharmacodynamic properties that can lead to drug-drug interactions (DDIs) that may go unnoticed in the inpatient setting. The purpose of this study was to identify the frequency of DDIs between medications prescribed for OUD and commonly used inpatient medications.</p><p><strong>Methods: </strong>This was a retrospective review of orders for buprenorphine, buprenorphine-naloxone, and methadone to identify potential DDIs. Adult inpatients with an order for one of these medications for OUD were included. Medication regimens were evaluated throughout the inpatient stay and on day of discharge for DDIs. DDIs were classified by severity and type of interaction (increased risk of QT prolongation, additive CNS effects/respiratory depression, and opioid withdrawal). The primary endpoint was the number of potential DDIs. Other endpoints included number of each classification/severity of DDI, duration of therapy of interacting medications, and modifications made to OUD medications because of DDIs.</p><p><strong>Results: </strong>A total of 102 patients were included, with 215 inpatient interactions and 83 interactions at discharge identified. While inpatient, 85% of patients were on an interacting medication, and 46% of patients were on an interacting medication at discharge. The most common classification of DDI was additive CNS effects/respiratory depression (68.8% inpatient, 50.6% discharge), followed by QT prolongation (24.2% inpatient, 45.8% discharge). The majority of DDIs were classified as requiring close monitoring rather than contraindicated.</p><p><strong>Discussion: </strong>There are opportunities to optimize the prescribing practices surrounding OUD medications in both the inpatient setting and at discharge to ensure patient safety.</p>","PeriodicalId":22710,"journal":{"name":"The Mental Health Clinician","volume":"11 4","pages":"231-237"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/00/72/i2168-9709-11-4-231.PMC8287868.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Mental Health Clinician","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.9740/mhc.2021.07.231","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/7/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Introduction: Medications used to treat OUD have common metabolic pathways and pharmacodynamic properties that can lead to drug-drug interactions (DDIs) that may go unnoticed in the inpatient setting. The purpose of this study was to identify the frequency of DDIs between medications prescribed for OUD and commonly used inpatient medications.
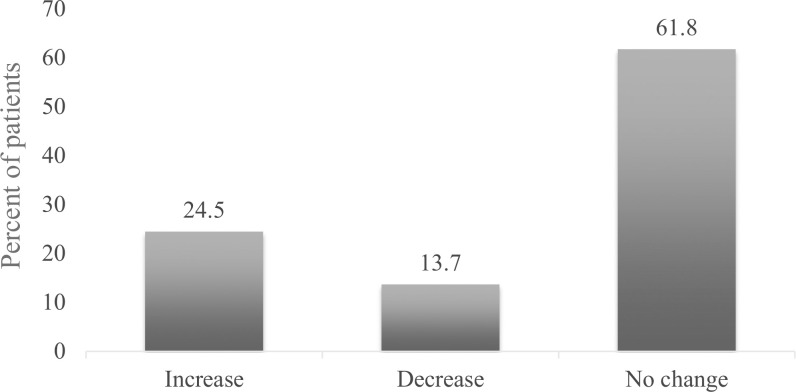
Methods: This was a retrospective review of orders for buprenorphine, buprenorphine-naloxone, and methadone to identify potential DDIs. Adult inpatients with an order for one of these medications for OUD were included. Medication regimens were evaluated throughout the inpatient stay and on day of discharge for DDIs. DDIs were classified by severity and type of interaction (increased risk of QT prolongation, additive CNS effects/respiratory depression, and opioid withdrawal). The primary endpoint was the number of potential DDIs. Other endpoints included number of each classification/severity of DDI, duration of therapy of interacting medications, and modifications made to OUD medications because of DDIs.
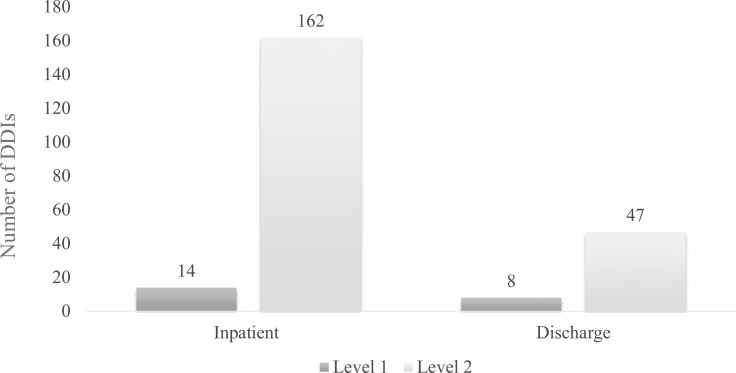
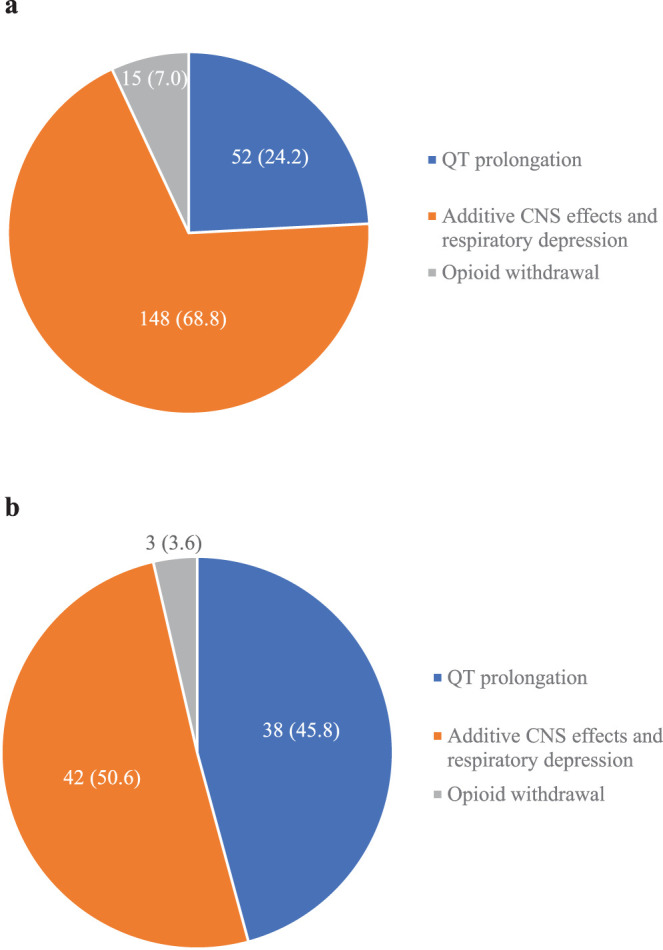
Results: A total of 102 patients were included, with 215 inpatient interactions and 83 interactions at discharge identified. While inpatient, 85% of patients were on an interacting medication, and 46% of patients were on an interacting medication at discharge. The most common classification of DDI was additive CNS effects/respiratory depression (68.8% inpatient, 50.6% discharge), followed by QT prolongation (24.2% inpatient, 45.8% discharge). The majority of DDIs were classified as requiring close monitoring rather than contraindicated.
Discussion: There are opportunities to optimize the prescribing practices surrounding OUD medications in both the inpatient setting and at discharge to ensure patient safety.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


