Mohammad A Sohail, Mohamed Hassanein, Hernan Rincon-Choles
{"title":"Ifosfamide-induced nephrogenic diabetes insipidus responsive to supraphysiologic doses of intravenous desmopressin.","authors":"Mohammad A Sohail, Mohamed Hassanein, Hernan Rincon-Choles","doi":"10.5414/CNCS110589","DOIUrl":null,"url":null,"abstract":"<p><p>Nephrogenic diabetes insipidus (DI) refers to the reduction in the ability of the kidney to concentrate urine, which can be caused by partial or complete resistance at the site of action of anti-diuretic hormone (ADH) in the collecting tubules. Ifosfamide-induced nephrogenic DI typically occurs concomitantly in patients who have other signs of tubular toxicity consistent with Fanconi syndrome including glucosuria, aminoaciduria, and hypophosphatemia. We present a case of a 36-year-old female with recurrent synovial cell sarcoma of the pleural membranes, treated with ifosfamide-based chemotherapy, who was admitted to the hospital for the management of polyuria, hypotension, as well as electrolyte derangements including hypokalemia, hypophosphatemia and non-anion gap metabolic acidosis, 1 week after receiving a cumulative ifosfamide dose of 7.5 g/m<sup>2</sup>. Nephrogenic DI was indicated by polyuria as well as a urine osmolality to plasma osmolality ratio of less than 1.5 following a trial of intravenous desmopressin, but the patient's acute kidney injury on presentation precluded the early employment of thiazides and non-steroidal anti-inflammatory drugs (NSAIDs). Instead, the patient's polyuria and urine osmolality improved only after the administration of repetitive supraphysiologic doses of intravenous desmopressin. Our case reiterates that patients with non-hereditary nephrogenic DI may have partial rather than complete resistance to ADH and highlights that desmopressin may be considered in patients with ifosfamide-induced nephrogenic DI to prevent severe volume depletion, especially in patients who have persistent symptomatic polyuria despite maintaining a careful fluid balance and pharmacological therapy with NSAIDs and diuretics, or if the patient's clinical condition precludes the use of these strategies.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"9 ","pages":"87-92"},"PeriodicalIF":0.0000,"publicationDate":"2021-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8259464/pdf/","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110589","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
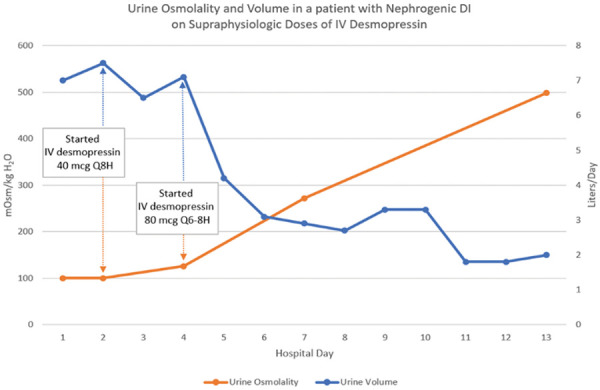
Nephrogenic diabetes insipidus (DI) refers to the reduction in the ability of the kidney to concentrate urine, which can be caused by partial or complete resistance at the site of action of anti-diuretic hormone (ADH) in the collecting tubules. Ifosfamide-induced nephrogenic DI typically occurs concomitantly in patients who have other signs of tubular toxicity consistent with Fanconi syndrome including glucosuria, aminoaciduria, and hypophosphatemia. We present a case of a 36-year-old female with recurrent synovial cell sarcoma of the pleural membranes, treated with ifosfamide-based chemotherapy, who was admitted to the hospital for the management of polyuria, hypotension, as well as electrolyte derangements including hypokalemia, hypophosphatemia and non-anion gap metabolic acidosis, 1 week after receiving a cumulative ifosfamide dose of 7.5 g/m2. Nephrogenic DI was indicated by polyuria as well as a urine osmolality to plasma osmolality ratio of less than 1.5 following a trial of intravenous desmopressin, but the patient's acute kidney injury on presentation precluded the early employment of thiazides and non-steroidal anti-inflammatory drugs (NSAIDs). Instead, the patient's polyuria and urine osmolality improved only after the administration of repetitive supraphysiologic doses of intravenous desmopressin. Our case reiterates that patients with non-hereditary nephrogenic DI may have partial rather than complete resistance to ADH and highlights that desmopressin may be considered in patients with ifosfamide-induced nephrogenic DI to prevent severe volume depletion, especially in patients who have persistent symptomatic polyuria despite maintaining a careful fluid balance and pharmacological therapy with NSAIDs and diuretics, or if the patient's clinical condition precludes the use of these strategies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


