Characterising the incidence and mode of visceral stent failure after fenestrated endovascular aneurysm repair (FEVAR).
IF 1.5
Q3 CARDIAC & CARDIOVASCULAR SYSTEMS
JRSM Cardiovascular Disease
Pub Date : 2021-04-28
eCollection Date: 2021-01-01
DOI:10.1177/20480040211012503
引用次数: 3
Abstract
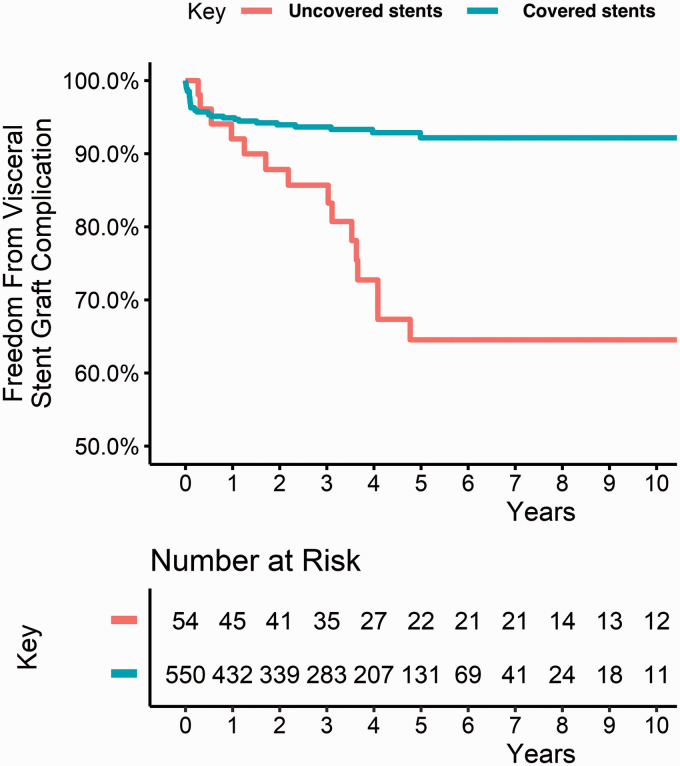
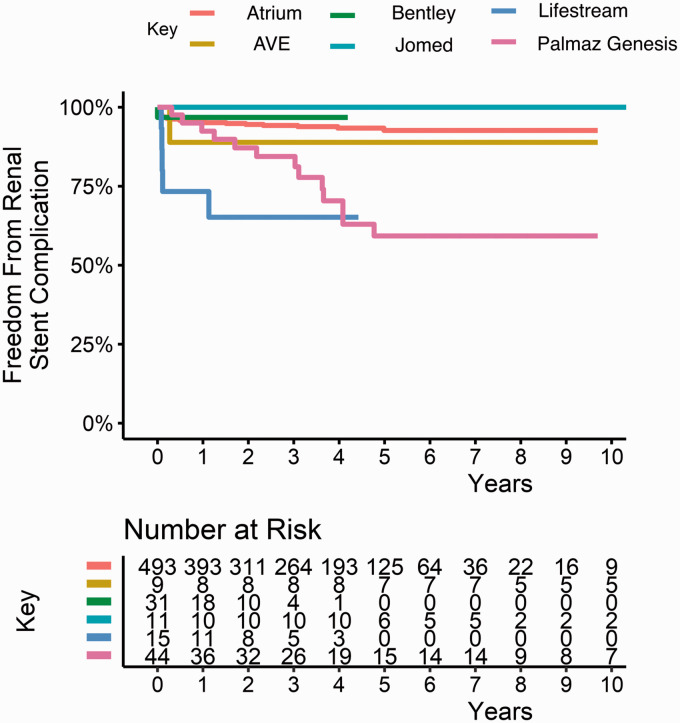
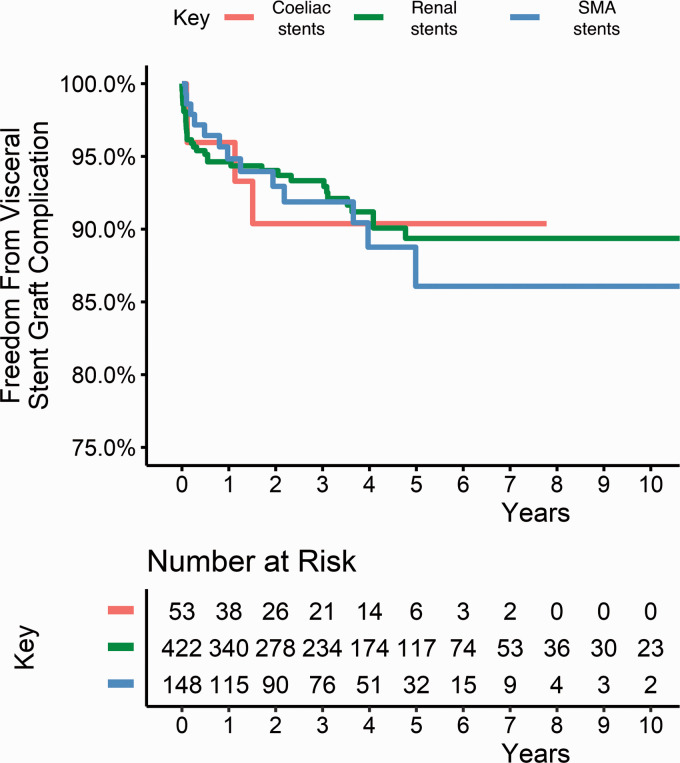
Background In FEVAR, visceral stents provide continuity and maintain perfusion between the main body of the stent and the respective visceral artery. The aim of this study was to characterise the incidence and mode of visceral stent failure (type Ic endoleak, type IIIa endoleak, stenosis/kink, fracture, crush and occlusion) after FEVAR in a large cohort of patients at a high-volume centre. Methods A retrospective review of visceral stents placed during FEVAR over 15 years (February 2003-December 2018) was performed. Kaplan-Meier analyses of freedom from visceral stent-related complications were performed. The outcomes between graft configurations of varying complexity were compared, as were the outcomes of different stent types and different visceral vessels. Results Visceral stent complications occurred in 47/236 patients (19.9%) and 54/653 stents (8.3%). Median follow up was 3.7 years (IQR 1.7–5.3 years). There was no difference in visceral stent complication rate between renal, SMA and coeliac arteries. Visceral stent complications were more frequent in more complex grafts compared to less complex grafts. Visceral stent complications were more frequent in uncovered stents compared to covered stents. Visceral stent-related endoleaks (type Ic and type IIIa) occurred exclusively around renal artery stents. The most common modes of failure with SMA stents were kinking and fracture, whereas with coeliac artery stents it was external crush. Conclusion Visceral stent complications after FEVAR are common and merit continued and close long-term surveillance. The mode of visceral stent failure varies across the vessels in which the stents are located.
开窗血管内动脉瘤修复(FEVAR)后内脏支架失效的发生率和模式。
背景:在FEVAR中,内脏支架在支架主体和各自的内脏动脉之间提供连续性和维持灌注。本研究的目的是在一个大容量中心的大队列患者中描述FEVAR后内脏支架失效的发生率和模式(Ic型内漏、IIIa型内漏、狭窄/扭曲、骨折、挤压和闭塞)。方法:回顾性回顾15年来(2003年2月- 2018年12月)FEVAR期间放置内脏支架的情况。对内脏支架相关并发症的自由进行Kaplan-Meier分析。比较了不同复杂程度的移植物构型之间的结果,以及不同支架类型和不同内脏血管的结果。结果:47/236例(19.9%)和54/653例(8.3%)发生了内脏支架并发症。中位随访3.7年(IQR为1.7-5.3年)。肾动脉、SMA动脉和腹腔动脉的内脏支架并发症发生率无差异。较复杂的移植比较不复杂的移植更容易出现内脏支架并发症。内脏支架并发症在未覆盖支架中比覆盖支架更常见。内脏支架相关的内漏(Ic型和IIIa型)仅发生在肾动脉支架周围。SMA支架最常见的失败模式是扭结和骨折,而腹腔动脉支架则是外挤压。结论:FEVAR后的内脏支架并发症是常见的,值得持续密切的长期监测。内脏支架失效的模式因支架所在血管的不同而不同。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


