{"title":"Sigmoid Volvulus: Diagnostic Modalities and Sigmoid Gangrene.","authors":"Sabri Selcuk Atamanalp, Esra Disci","doi":"10.5152/eurasianjmed.2021.21101","DOIUrl":null,"url":null,"abstract":"In SV, abdominal pain/tenderness, obstipation, and asymmetrical abdominal distention (Figure 1a), which are described as the volvulus triad, are observed in 52%-99% of patients.1,3 In our evaluation, these clinical features were found in 98.9%, 96.6%, and 92.4% of patients, respectively. Other clinical features are vomiting, hyperkinetic or hypokinetic bowel sounds, empty rectum or melanotic stool, and shock.1,3 In endemic regions, the determination of the abovementioned features in a middle aged or elderly man is generally suggestive of SV.3 Plain abdominal X-ray radiography demonstrating an omega-shaped sigmoid colon with small intestinal air-fluid levels is diagnostic in 25%-90% of patients (Figure 1b)1,3; this was observed in 68.2% of our patients. Nevertheless, the diagnostic values of computerized tomography (CT) and magnetic resonance imaging (MRI) are generally reported to be over 90%. In CT and MRI, the pathognomonic finding of SV is mesenteric whirl sign arising from rotated sigmoid mesentery in addition to the dilated sigmoid colon and small intestinal air-fluid levels (Figures 1c, 1d).3 In our evaluation, the diagnostic accuracy of CT and MRI were 97.3% and 95.6%, respectively. Endoscopic sign of SV is a spiral torsion of the lumen, usually 20-30 cm from the anal verge (Figure 1e). Endoscopy is diagnostic in 76%-100% of patients3; this was observed in 98.7% of our patients. When CT, MRI, or endoscopy are not used, SV is easily misdiagnosed as an intestinal obstruction, which generally requires an emergency laparotomy.1,3","PeriodicalId":517142,"journal":{"name":"The Eurasian Journal of Medicine","volume":" ","pages":"166-167"},"PeriodicalIF":0.0000,"publicationDate":"2021-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8184029/pdf/","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Eurasian Journal of Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5152/eurasianjmed.2021.21101","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 4
Abstract
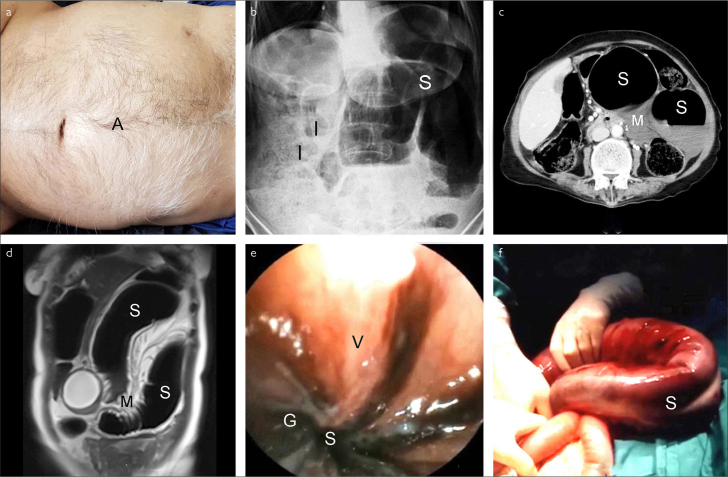
In SV, abdominal pain/tenderness, obstipation, and asymmetrical abdominal distention (Figure 1a), which are described as the volvulus triad, are observed in 52%-99% of patients.1,3 In our evaluation, these clinical features were found in 98.9%, 96.6%, and 92.4% of patients, respectively. Other clinical features are vomiting, hyperkinetic or hypokinetic bowel sounds, empty rectum or melanotic stool, and shock.1,3 In endemic regions, the determination of the abovementioned features in a middle aged or elderly man is generally suggestive of SV.3 Plain abdominal X-ray radiography demonstrating an omega-shaped sigmoid colon with small intestinal air-fluid levels is diagnostic in 25%-90% of patients (Figure 1b)1,3; this was observed in 68.2% of our patients. Nevertheless, the diagnostic values of computerized tomography (CT) and magnetic resonance imaging (MRI) are generally reported to be over 90%. In CT and MRI, the pathognomonic finding of SV is mesenteric whirl sign arising from rotated sigmoid mesentery in addition to the dilated sigmoid colon and small intestinal air-fluid levels (Figures 1c, 1d).3 In our evaluation, the diagnostic accuracy of CT and MRI were 97.3% and 95.6%, respectively. Endoscopic sign of SV is a spiral torsion of the lumen, usually 20-30 cm from the anal verge (Figure 1e). Endoscopy is diagnostic in 76%-100% of patients3; this was observed in 98.7% of our patients. When CT, MRI, or endoscopy are not used, SV is easily misdiagnosed as an intestinal obstruction, which generally requires an emergency laparotomy.1,3

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


