Leonardo Caroti, Giuseppe Cestone, Lorenzo Di Maria, Marco Allinovi, Vicenzo Li Marzi, Sergio Serni, Calogero Lino Cirami
{"title":"Hemolytic uremic syndrome and kidney transplantation in uncontrolled donation after circulatory death (DCD): A two-case report.","authors":"Leonardo Caroti, Giuseppe Cestone, Lorenzo Di Maria, Marco Allinovi, Vicenzo Li Marzi, Sergio Serni, Calogero Lino Cirami","doi":"10.5414/CNCS110434","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Hemolytic uremic syndrome (HUS) is a rare disease characterized by microangiopathic hemolysis, thrombocytopenia, and renal involvement. Complement-mediated atypical HUS (aHUS) is a result of genetic defects in the alternative complement pathway components or regulators. The introduction of eculizumab has improved renal and overall survival of aHUS patients. Nowadays, given organ shortage, it is necessary to consider kidney transplantation (KT) even in protocols with a high risk of HUS recurrence, such as from donation after circulatory death (DCD) donors. Here, we describe two patients with HUS who underwent a KT from an uncontrolled DCD (uDCD).</p><p><strong>Case summary: </strong>The first patient, affected by aHUS due to a heterozygous deletion in CFHR3-CFHR1 and a novel heterozygous variant in CFHR5 gene, underwent a KT with eculizumab prophylaxis. The patient did not experience a post-transplant aHUS recurrence. The second patient, who experienced an HUS episode characterized by a hypertensive crisis and with no underlying mutations in complement system genes, underwent a KT without eculizumab prophylaxis. At day 5, anti-complement treatment commenced due to hematological signs of thrombotic microangiopathy (TMA). After the introduction of eculizumab, we observed a stabilization of kidney function and hematological remission.</p><p><strong>Conclusion: </strong>We present herein two different patients with HUS who both underwent successful KT from uDCD donation under the umbrella of eculizumab therapy. Taking into account the importance of increasing the number of organs available for transplantation, uDCD could represent an additional resource in this subset of HUS patients.</p>","PeriodicalId":10398,"journal":{"name":"Clinical Nephrology. Case Studies","volume":"9 ","pages":"59-66"},"PeriodicalIF":0.0000,"publicationDate":"2021-05-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8170123/pdf/","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Nephrology. Case Studies","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5414/CNCS110434","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Hemolytic uremic syndrome (HUS) is a rare disease characterized by microangiopathic hemolysis, thrombocytopenia, and renal involvement. Complement-mediated atypical HUS (aHUS) is a result of genetic defects in the alternative complement pathway components or regulators. The introduction of eculizumab has improved renal and overall survival of aHUS patients. Nowadays, given organ shortage, it is necessary to consider kidney transplantation (KT) even in protocols with a high risk of HUS recurrence, such as from donation after circulatory death (DCD) donors. Here, we describe two patients with HUS who underwent a KT from an uncontrolled DCD (uDCD).
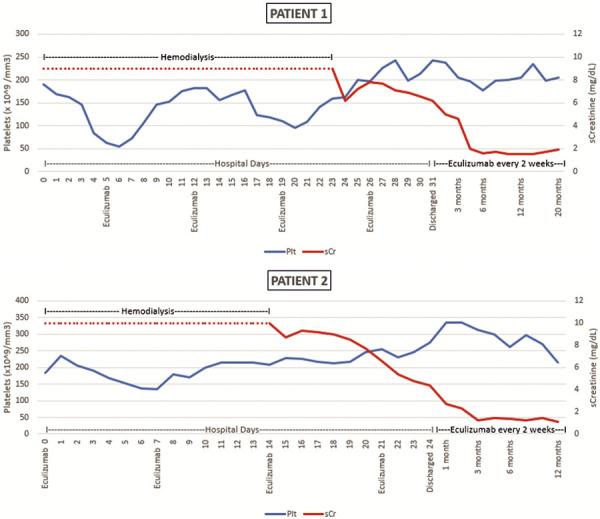
Case summary: The first patient, affected by aHUS due to a heterozygous deletion in CFHR3-CFHR1 and a novel heterozygous variant in CFHR5 gene, underwent a KT with eculizumab prophylaxis. The patient did not experience a post-transplant aHUS recurrence. The second patient, who experienced an HUS episode characterized by a hypertensive crisis and with no underlying mutations in complement system genes, underwent a KT without eculizumab prophylaxis. At day 5, anti-complement treatment commenced due to hematological signs of thrombotic microangiopathy (TMA). After the introduction of eculizumab, we observed a stabilization of kidney function and hematological remission.
Conclusion: We present herein two different patients with HUS who both underwent successful KT from uDCD donation under the umbrella of eculizumab therapy. Taking into account the importance of increasing the number of organs available for transplantation, uDCD could represent an additional resource in this subset of HUS patients.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


