Evaluating the Clinical Utility of Routine Sentinel Lymph Node Biopsy and the Value of Adjuvant Chemotherapy in Elderly Patients Diagnosed With Oestrogen Receptor Positive, Clinically Node Negative Breast Cancer.
Matthew G Davey, Éanna J Ryan, Daniel Burke, Kevin McKevitt, Peter F McAnena, Michael J Kerin, Aoife J Lowery
{"title":"Evaluating the Clinical Utility of Routine Sentinel Lymph Node Biopsy and the Value of Adjuvant Chemotherapy in Elderly Patients Diagnosed With Oestrogen Receptor Positive, Clinically Node Negative Breast Cancer.","authors":"Matthew G Davey, Éanna J Ryan, Daniel Burke, Kevin McKevitt, Peter F McAnena, Michael J Kerin, Aoife J Lowery","doi":"10.1177/11782234211022203","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Sentinel lymph node biopsy (SLNB) provides staging information and guides adjuvant therapy in early breast cancer (EBC). Routine SLNB in oncogeriatricians with low-risk EBC remains controversial.</p><p><strong>Aims: </strong>To evaluate axillary management in elderly patients diagnosed with oestrogen receptor positive (ER+), clinically lymph node negative (cLN-) EBC, and to assess whether SLNB affects further axillary management or adjuvant chemotherapy (ACTX) decision making.</p><p><strong>Methods: </strong>Female patients aged > 65 years, diagnosed with ER+, human epidermal growth factor receptor-2 negative (HER2-), and cLN- breast cancer (BC), who underwent surgery and SLNB were included. Clinicopathological predictors of ACTX and completion axillary lymph node dissection (CALND) were determined. Kaplan-Meier analyses assessed survival outcomes.</p><p><strong>Results: </strong>A total of 253 patients were included (median age: 72 years, range: 66-90), all underwent SLNB; 50 (19.8%) had lymphatic metastasis on SLNB (SLNB+). Of these, 19 proceeded to CALND (38.0%), 10 (52.6%) of whom had further axillary disease (ALND+). 20 of the 50 SLNB+ patients received ACTX (40.0%) as did 31 of the 203 SLNB- patients (15.2%) (<i>P</i> < .001). Oncotype DX (ODX) testing was utilized in 82 cases (32.8%). Younger age (<i>P</i> < .001), SLNB+ (<i>P</i> < .001) and ODX score (<i>P</i> = .003) were all associated with ACTX prescription. ODX > 25 (OR: 4.37, 95% CI: 1.38-13.80, <i>P</i> = .012) independently predicted receiving ACTX. Receiving ACTX and proceeding to CALND did not improve disease-free (<i>P</i> = .485 and <i>P</i> = .345) or overall survival (<i>P</i> = .981 and <i>P</i> = .646).</p><p><strong>Conclusions: </strong>Routine SNLB may not be necessary in elderly patients diagnosed with ER+, cLN- EBC. Future oncogeriatric practice is likely to see genomic testing guiding ACTX prescription in this group.</p>","PeriodicalId":9163,"journal":{"name":"Breast Cancer : Basic and Clinical Research","volume":"15 ","pages":"11782234211022203"},"PeriodicalIF":1.9000,"publicationDate":"2021-06-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/11782234211022203","citationCount":"4","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Breast Cancer : Basic and Clinical Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/11782234211022203","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 4
Abstract
Background: Sentinel lymph node biopsy (SLNB) provides staging information and guides adjuvant therapy in early breast cancer (EBC). Routine SLNB in oncogeriatricians with low-risk EBC remains controversial.
Aims: To evaluate axillary management in elderly patients diagnosed with oestrogen receptor positive (ER+), clinically lymph node negative (cLN-) EBC, and to assess whether SLNB affects further axillary management or adjuvant chemotherapy (ACTX) decision making.
Methods: Female patients aged > 65 years, diagnosed with ER+, human epidermal growth factor receptor-2 negative (HER2-), and cLN- breast cancer (BC), who underwent surgery and SLNB were included. Clinicopathological predictors of ACTX and completion axillary lymph node dissection (CALND) were determined. Kaplan-Meier analyses assessed survival outcomes.
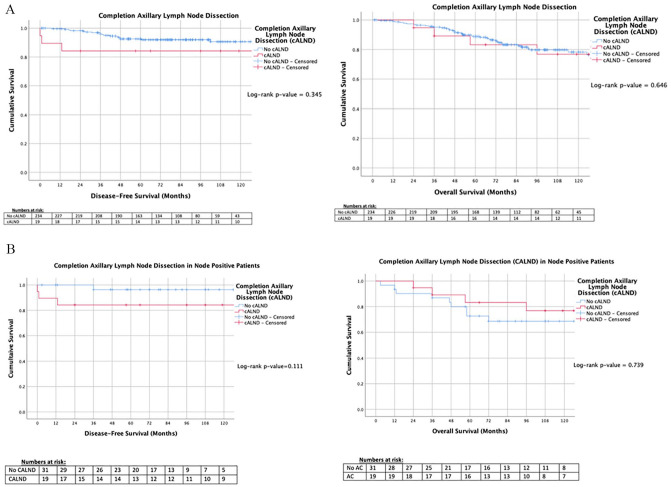
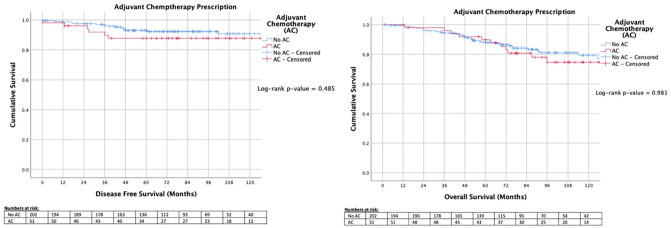
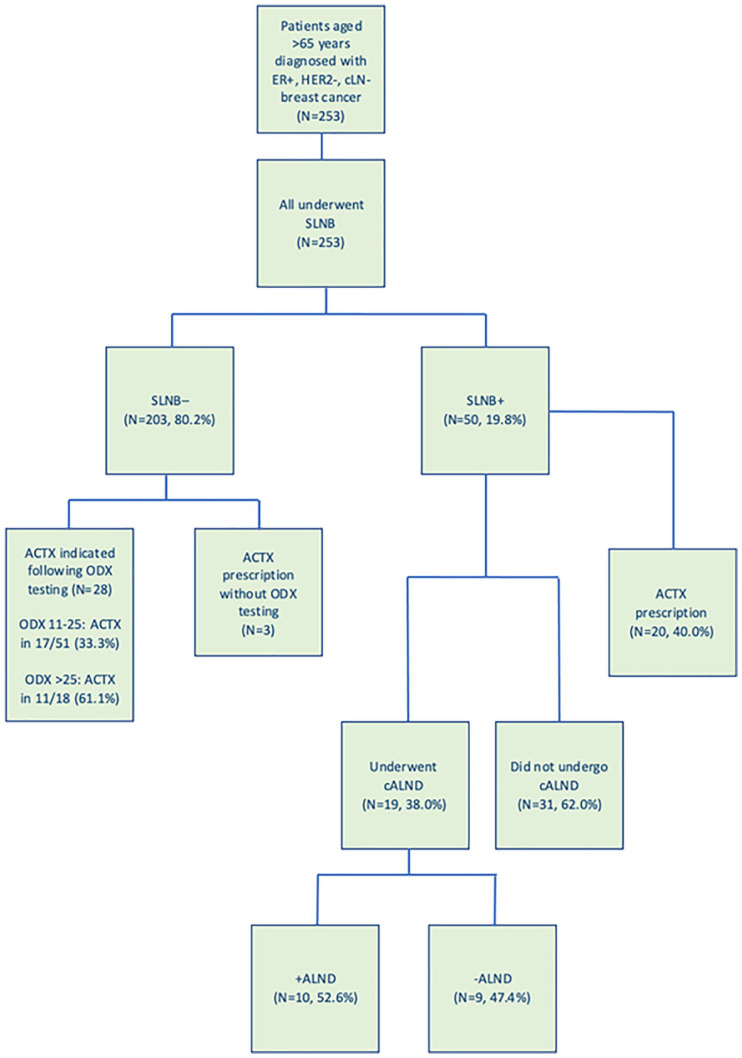
Results: A total of 253 patients were included (median age: 72 years, range: 66-90), all underwent SLNB; 50 (19.8%) had lymphatic metastasis on SLNB (SLNB+). Of these, 19 proceeded to CALND (38.0%), 10 (52.6%) of whom had further axillary disease (ALND+). 20 of the 50 SLNB+ patients received ACTX (40.0%) as did 31 of the 203 SLNB- patients (15.2%) (P < .001). Oncotype DX (ODX) testing was utilized in 82 cases (32.8%). Younger age (P < .001), SLNB+ (P < .001) and ODX score (P = .003) were all associated with ACTX prescription. ODX > 25 (OR: 4.37, 95% CI: 1.38-13.80, P = .012) independently predicted receiving ACTX. Receiving ACTX and proceeding to CALND did not improve disease-free (P = .485 and P = .345) or overall survival (P = .981 and P = .646).
Conclusions: Routine SNLB may not be necessary in elderly patients diagnosed with ER+, cLN- EBC. Future oncogeriatric practice is likely to see genomic testing guiding ACTX prescription in this group.
期刊介绍:
Breast Cancer: Basic and Clinical Research is an international, open access, peer-reviewed, journal which considers manuscripts on all areas of breast cancer research and treatment. We welcome original research, short notes, case studies and review articles related to breast cancer-related research. Specific areas of interest include, but are not limited to, breast cancer sub types, pathobiology, metastasis, genetics and epigenetics, mammary gland biology, breast cancer models, prevention, detection, therapy and clinical interventions, and epidemiology and population genetics.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


