Maren Shapiro, Phillip Romanski, Ann Thomas, Andrea Lanes, Elena Yanushpolsky
{"title":"Low dose hCG supplementation in a Gn-RH-agonist trigger protocol is associated with worse pregnancy outcomes: a retrospective cohort study.","authors":"Maren Shapiro, Phillip Romanski, Ann Thomas, Andrea Lanes, Elena Yanushpolsky","doi":"10.1186/s40738-021-00104-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>A number of studies have looked at dual triggers with hCG and GnRH agonist (GnRHa) in varying doses, but the question remains: what is the optimal dose of hCG to minimize ovarian hyperstimulation syndrome (OHSS) and still offer adequate pregnancy rates? The purpose of this study was to compare pregnancy and OHSS rates following dual trigger for oocyte maturation with GnRHa and a low-dose hCG versus hCG alone. A secondary objective was the assess pregnancy outcomes in subsequent frozen cycles for the same population.</p><p><strong>Methods: </strong>A total of 963 women < 41 years old, with a BMI 18-40 kg/m<sup>2</sup> and an AMH > 2 ng/mL who underwent fresh autologous in vitro fertilization (IVF) with GnRH antagonist protocol at a University-based fertility center were included in this retrospective cohort study. Those who received a low dose dual trigger with hCG (1000u) and GnRHa (2 mg) were compared to those who received hCG alone (10,000u hCG/250-500 μg Ovidrel). Differences in implantation rates, pregnancy, live birth, and OHSS were investigated.</p><p><strong>Results: </strong>The dual trigger group was younger (mean 33.6 vs 34.1 years), had a higher AMH (6.3 vs 4.9 ng/mL,) more oocytes retrieved (18.1 vs 14.9) and a higher fertilized oocyte rate (80% vs 77%) compared with the hCG only group. Yet, the dual trigger group had a lower probability of clinical pregnancy (gestational sac, 43.4% vs 52.8%) and live birth (33.4% vs 45.8%), all of which were statistically significant. There were 3 cases of OHSS, all in the hCG-only trigger group. In subsequent frozen cycles, pregnancy rates were comparable between the two groups.</p><p><strong>Conclusions: </strong>The dual trigger group had a better prognosis based on age and AMH levels and had better stimulation outcomes, but significantly worse pregnancy outcomes, suggesting the low dose hCG (1000u) in the dual trigger may not have provided adequate luteal support, compared to an hCG-only trigger (10,000u hCG/250-500 μg Ovidrel). Interestingly, the pregnancy rates were comparable in subsequent frozen cycles, further supporting the hypothesis that the issue lies in inadequate luteal phase support, rather than embryo quality. Based on these findings, our program has changed the protocol to 1500u of hCG in a dual trigger.</p>","PeriodicalId":87254,"journal":{"name":"Fertility research and practice","volume":"7 1","pages":"12"},"PeriodicalIF":0.0000,"publicationDate":"2021-05-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8161625/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Fertility research and practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40738-021-00104-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: A number of studies have looked at dual triggers with hCG and GnRH agonist (GnRHa) in varying doses, but the question remains: what is the optimal dose of hCG to minimize ovarian hyperstimulation syndrome (OHSS) and still offer adequate pregnancy rates? The purpose of this study was to compare pregnancy and OHSS rates following dual trigger for oocyte maturation with GnRHa and a low-dose hCG versus hCG alone. A secondary objective was the assess pregnancy outcomes in subsequent frozen cycles for the same population.
Methods: A total of 963 women < 41 years old, with a BMI 18-40 kg/m2 and an AMH > 2 ng/mL who underwent fresh autologous in vitro fertilization (IVF) with GnRH antagonist protocol at a University-based fertility center were included in this retrospective cohort study. Those who received a low dose dual trigger with hCG (1000u) and GnRHa (2 mg) were compared to those who received hCG alone (10,000u hCG/250-500 μg Ovidrel). Differences in implantation rates, pregnancy, live birth, and OHSS were investigated.
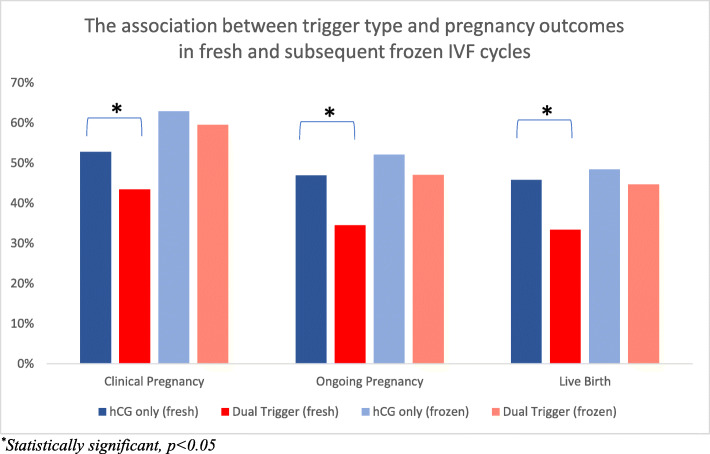
Results: The dual trigger group was younger (mean 33.6 vs 34.1 years), had a higher AMH (6.3 vs 4.9 ng/mL,) more oocytes retrieved (18.1 vs 14.9) and a higher fertilized oocyte rate (80% vs 77%) compared with the hCG only group. Yet, the dual trigger group had a lower probability of clinical pregnancy (gestational sac, 43.4% vs 52.8%) and live birth (33.4% vs 45.8%), all of which were statistically significant. There were 3 cases of OHSS, all in the hCG-only trigger group. In subsequent frozen cycles, pregnancy rates were comparable between the two groups.
Conclusions: The dual trigger group had a better prognosis based on age and AMH levels and had better stimulation outcomes, but significantly worse pregnancy outcomes, suggesting the low dose hCG (1000u) in the dual trigger may not have provided adequate luteal support, compared to an hCG-only trigger (10,000u hCG/250-500 μg Ovidrel). Interestingly, the pregnancy rates were comparable in subsequent frozen cycles, further supporting the hypothesis that the issue lies in inadequate luteal phase support, rather than embryo quality. Based on these findings, our program has changed the protocol to 1500u of hCG in a dual trigger.
背景:许多研究已经研究了不同剂量的hCG和GnRH激动剂(GnRHa)的双重触发,但问题仍然存在:hCG的最佳剂量是多少才能最大限度地减少卵巢过度刺激综合征(OHSS)并仍然提供足够的怀孕率?本研究的目的是比较GnRHa和低剂量hCG与单独hCG双重触发卵母细胞成熟后的妊娠率和OHSS率。第二个目的是评估同一人群后续冷冻周期的妊娠结局。方法:在一所大学生育中心接受新鲜体外受精(IVF)和GnRH拮抗剂方案的963名AMH > 2 ng/mL的妇女2纳入本回顾性队列研究。将接受低剂量hCG (1000u)和GnRHa (2mg)双重触发治疗的患者与单独接受hCG (10000 u hCG/250-500 μg Ovidrel)治疗的患者进行比较。研究着床率、妊娠、活产和OHSS的差异。结果:与仅hCG组相比,双触发组更年轻(平均33.6 vs 34.1岁),AMH更高(6.3 vs 4.9 ng/mL),回收的卵母细胞更多(18.1 vs 14.9),受精卵率更高(80% vs 77%)。但双触发组临床妊娠(胎囊,43.4% vs 52.8%)和活产(33.4% vs 45.8%)的概率较低,差异均有统计学意义。OHSS 3例,均为单纯hcg触发组。在随后的冷冻周期中,两组之间的妊娠率相当。结论:双触发组基于年龄和AMH水平的预后更好,刺激结果更好,但妊娠结局明显差,提示双触发组低剂量hCG (1000u)可能没有提供足够的黄体支持,而单触发组(10000 u hCG/250 ~ 500 μg Ovidrel)。有趣的是,在随后的冷冻周期中,怀孕率是相当的,这进一步支持了问题在于黄体期支持不足而不是胚胎质量的假设。基于这些发现,我们的项目将方案改为1500u hCG双触发。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


