Ultrasound-Guided Local Anesthetic Infiltration Between the Popliteal Artery and the Capsule of the Posterior Knee (IPACK) Block for Primary Total Knee Arthroplasty: A Systematic Review of Randomized Controlled Trials.
Ryan S D'Souza, Brendan J Langford, David A Olsen, Rebecca L Johnson
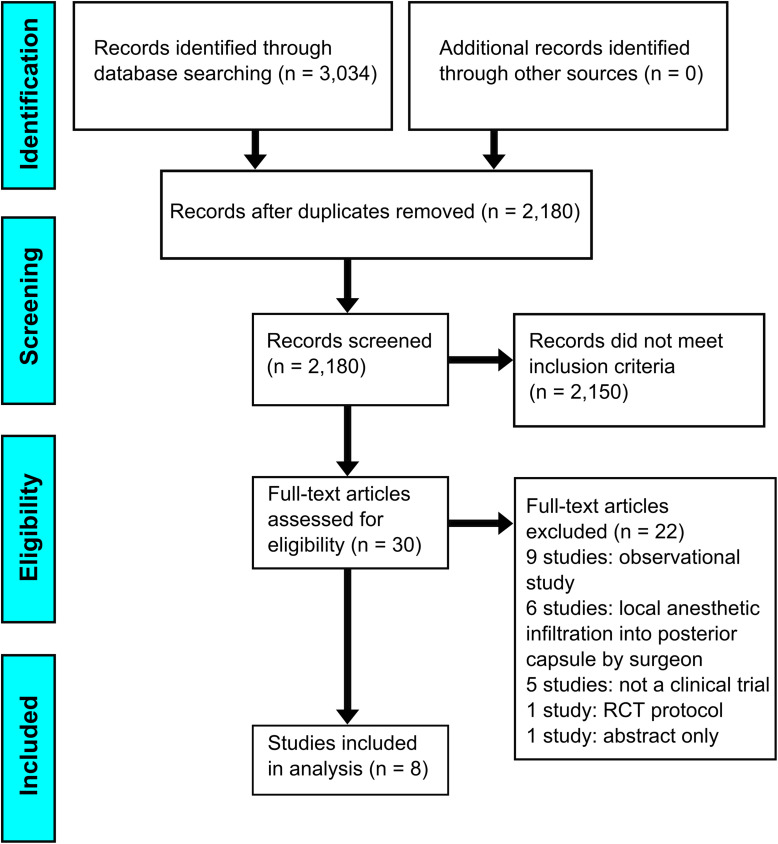
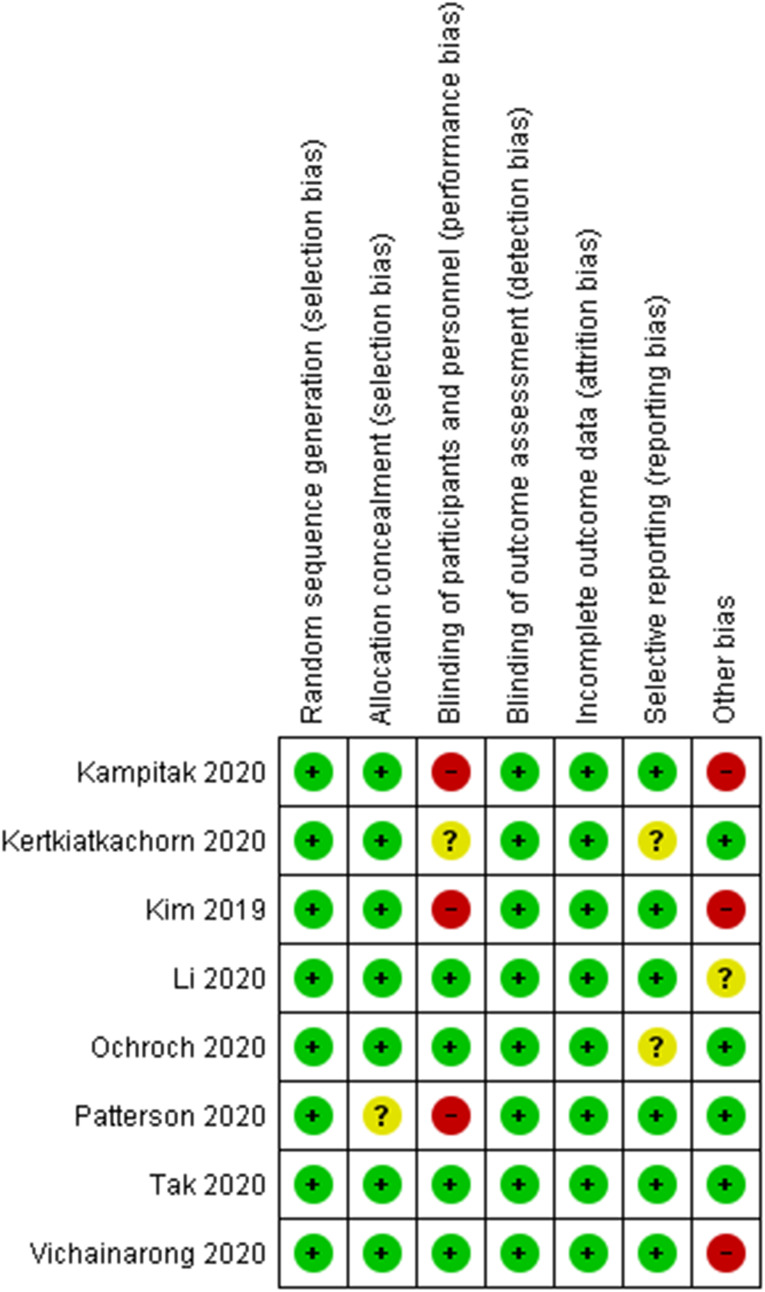
{"title":"Ultrasound-Guided Local Anesthetic Infiltration Between the Popliteal Artery and the Capsule of the Posterior Knee (IPACK) Block for Primary Total Knee Arthroplasty: A Systematic Review of Randomized Controlled Trials.","authors":"Ryan S D'Souza, Brendan J Langford, David A Olsen, Rebecca L Johnson","doi":"10.2147/LRA.S303827","DOIUrl":null,"url":null,"abstract":"<p><p>Posterior knee pain after total knee arthroplasty (TKA) is common despite multimodal analgesia and regional anesthesia use. This review included randomized controlled trials (RCTs) comparing analgesic outcomes after inclusion of local anesthetic infiltration between the popliteal artery and capsule of the knee (iPACK) block versus pathways without iPACK. Electronic databases (MEDLINE, Cochrane Library, Web of Science, Scopus) were searched from inception to 10/11/2020. Eligible studies evaluated iPACK use on primary outcomes: opioid consumption and pain scores with movement. Secondary outcomes included rest pain, patient satisfaction, length of stay (LOS), gait distance, knee range of motion (ROM), and complications. Bias and quality were appraised using the Cochrane Risk of Bias tool and Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) guidelines. Eight RCTs (777 patients) were included. iPACK block use demonstrated similar opioid consumption in the PACU (4/7 RCTs) and 24 hours after TKA (5/7 RCTs) compared to without iPACK (moderate-quality GRADE evidence). Additionally, iPACK block use demonstrated lower movement pain scores in PACU (3/5 RCTs) but similar or higher pain scores after 24 hours (5/7 RCTs; low-quality GRADE evidence). Studies consistently reported no difference in gait distance (4/4 RCTs) or complications (7/7 RCTs) between treatment arms (high-quality GRADE evidence), although differing effect estimates were observed with resting pain, satisfaction, LOS, and knee ROM. This review provides a foundation of knowledge on iPACK efficacy. While evidence does not currently support widespread inclusion of iPACK within enhanced recovery pathways for TKA, limitations suggest further study is warranted.</p>","PeriodicalId":18203,"journal":{"name":"Local and Regional Anesthesia","volume":"14 ","pages":"85-98"},"PeriodicalIF":1.9000,"publicationDate":"2021-05-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/45/41/lra-14-85.PMC8126972.pdf","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Local and Regional Anesthesia","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/LRA.S303827","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2021/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 13
Abstract
Posterior knee pain after total knee arthroplasty (TKA) is common despite multimodal analgesia and regional anesthesia use. This review included randomized controlled trials (RCTs) comparing analgesic outcomes after inclusion of local anesthetic infiltration between the popliteal artery and capsule of the knee (iPACK) block versus pathways without iPACK. Electronic databases (MEDLINE, Cochrane Library, Web of Science, Scopus) were searched from inception to 10/11/2020. Eligible studies evaluated iPACK use on primary outcomes: opioid consumption and pain scores with movement. Secondary outcomes included rest pain, patient satisfaction, length of stay (LOS), gait distance, knee range of motion (ROM), and complications. Bias and quality were appraised using the Cochrane Risk of Bias tool and Grading of Recommendations, Assessment, Development, and Evaluations (GRADE) guidelines. Eight RCTs (777 patients) were included. iPACK block use demonstrated similar opioid consumption in the PACU (4/7 RCTs) and 24 hours after TKA (5/7 RCTs) compared to without iPACK (moderate-quality GRADE evidence). Additionally, iPACK block use demonstrated lower movement pain scores in PACU (3/5 RCTs) but similar or higher pain scores after 24 hours (5/7 RCTs; low-quality GRADE evidence). Studies consistently reported no difference in gait distance (4/4 RCTs) or complications (7/7 RCTs) between treatment arms (high-quality GRADE evidence), although differing effect estimates were observed with resting pain, satisfaction, LOS, and knee ROM. This review provides a foundation of knowledge on iPACK efficacy. While evidence does not currently support widespread inclusion of iPACK within enhanced recovery pathways for TKA, limitations suggest further study is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


