Lina Driouk, Robert Schmitt, Anke Peters, Sabine Heine, Hermann Josef Girschick, Brigitte Strahm, Charlotte M Niemeyer, Carsten Speckmann
{"title":"Daratumumab therapy for post-HSCT immune-mediated cytopenia: experiences from two pediatric cases and review of literature.","authors":"Lina Driouk, Robert Schmitt, Anke Peters, Sabine Heine, Hermann Josef Girschick, Brigitte Strahm, Charlotte M Niemeyer, Carsten Speckmann","doi":"10.1186/s40348-021-00114-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Immune-mediated cytopenias (AIC) are challenging complications following allogeneic hematopoietic stem cell transplantation (HSCT). While broad-acting immunosuppressive agents like corticosteroids are often standard of care, several novel therapies which target specific immunological pathways have recently been developed and provide hope for patients with steroid-refractory courses and may limit long-term toxicity. The successful off-label use of the plasma cell depleting anti-CD38 antibody daratumumab was published in several case reports, suggesting efficacy, i.e., in patients with antibody-mediated AIC refractory to previous B cell depletion. We want to share our experience with two children, whom we treated with daratumumab, including one fatal course with uncontrolled disease. Given the absence of substantial data from HSCT registries or prospective trials, we furthermore provide a critical review of the literature on daratumumab treatment of AIC.</p><p><strong>Case presentations: </strong>Patient 1 (P1), an 11-year-old girl with lipopolysaccharide-responsive and beige-like anchor protein (LRBA) deficiency who developed immune-mediated thrombocytopenia (AIT) from day +58 after HSCT, showed a complete response to daratumumab after the fourth of six total daratumumab doses. She remains transfusion independent for over a year of follow-up. Previously, her thrombocytopenia was refractory to corticosteroids, rituximab, intravenous immunoglobulins (IVIG), eltrombopag, cyclosporine A, and sirolimus. Patient 2 (P2), a 6-year-old boy with CD40 ligand (CD40L) deficiency, developed both AIT and hemolytic anemia (AIHA) after HSCT on days +58 and +83, respectively, and was also treated with daratumumab after being previously refractory to prednisolone, rituximab, and IVIG. Yet, he did neither respond to daratumumab nor the concomitantly administered methyprednisolone pulse, plasmapheresis, and eculizumab and succumbed due to refractory disease.</p><p><strong>Conclusion: </strong>Reviewing the literature on the use of daratumumab for refractory AIC post-HSCT, we consider daratumumab a promising agent for this life-threatening disorder: ten of the twelve patients reached transfusion independency in the literature. However, treatment failures are likely to be underreported. Thus, controlled trials are needed to explore the safety and efficacy of daratumumab in this rare post-HSCT complication.</p>","PeriodicalId":74215,"journal":{"name":"Molecular and cellular pediatrics","volume":"8 1","pages":"5"},"PeriodicalIF":2.4000,"publicationDate":"2021-04-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40348-021-00114-y","citationCount":"11","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Molecular and cellular pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40348-021-00114-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 11
Abstract
Background: Immune-mediated cytopenias (AIC) are challenging complications following allogeneic hematopoietic stem cell transplantation (HSCT). While broad-acting immunosuppressive agents like corticosteroids are often standard of care, several novel therapies which target specific immunological pathways have recently been developed and provide hope for patients with steroid-refractory courses and may limit long-term toxicity. The successful off-label use of the plasma cell depleting anti-CD38 antibody daratumumab was published in several case reports, suggesting efficacy, i.e., in patients with antibody-mediated AIC refractory to previous B cell depletion. We want to share our experience with two children, whom we treated with daratumumab, including one fatal course with uncontrolled disease. Given the absence of substantial data from HSCT registries or prospective trials, we furthermore provide a critical review of the literature on daratumumab treatment of AIC.
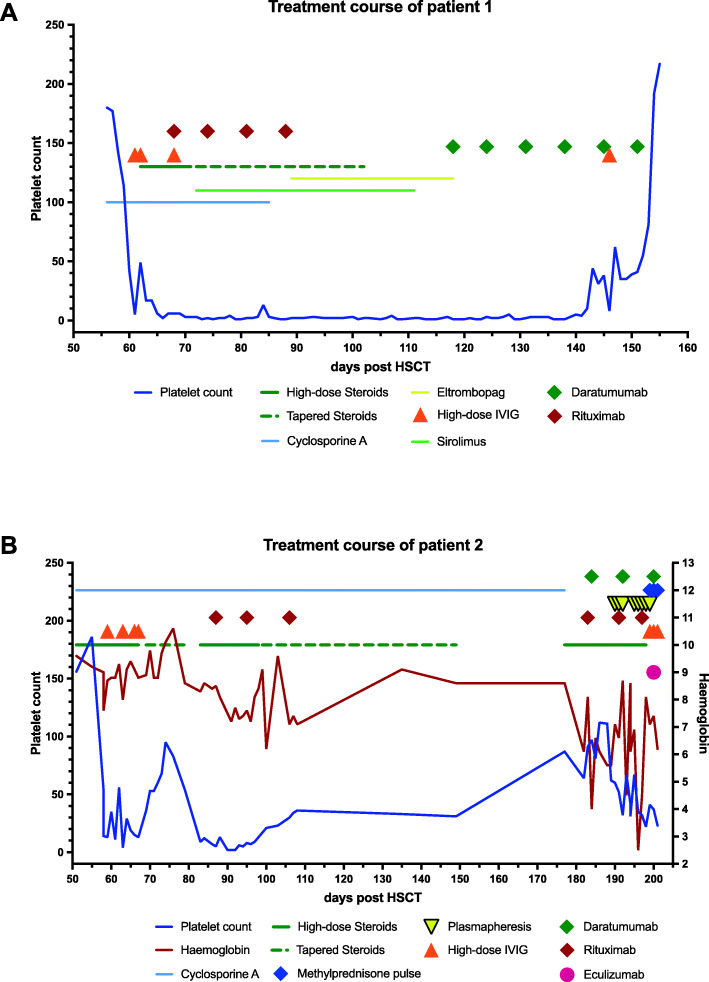
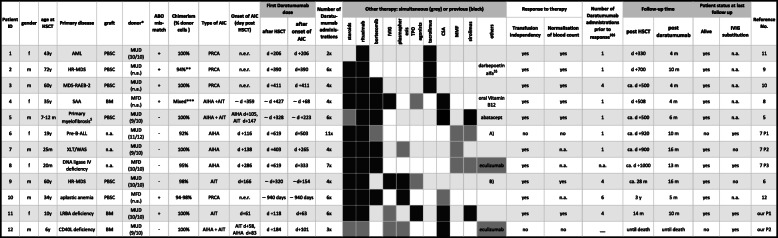
Case presentations: Patient 1 (P1), an 11-year-old girl with lipopolysaccharide-responsive and beige-like anchor protein (LRBA) deficiency who developed immune-mediated thrombocytopenia (AIT) from day +58 after HSCT, showed a complete response to daratumumab after the fourth of six total daratumumab doses. She remains transfusion independent for over a year of follow-up. Previously, her thrombocytopenia was refractory to corticosteroids, rituximab, intravenous immunoglobulins (IVIG), eltrombopag, cyclosporine A, and sirolimus. Patient 2 (P2), a 6-year-old boy with CD40 ligand (CD40L) deficiency, developed both AIT and hemolytic anemia (AIHA) after HSCT on days +58 and +83, respectively, and was also treated with daratumumab after being previously refractory to prednisolone, rituximab, and IVIG. Yet, he did neither respond to daratumumab nor the concomitantly administered methyprednisolone pulse, plasmapheresis, and eculizumab and succumbed due to refractory disease.
Conclusion: Reviewing the literature on the use of daratumumab for refractory AIC post-HSCT, we consider daratumumab a promising agent for this life-threatening disorder: ten of the twelve patients reached transfusion independency in the literature. However, treatment failures are likely to be underreported. Thus, controlled trials are needed to explore the safety and efficacy of daratumumab in this rare post-HSCT complication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


