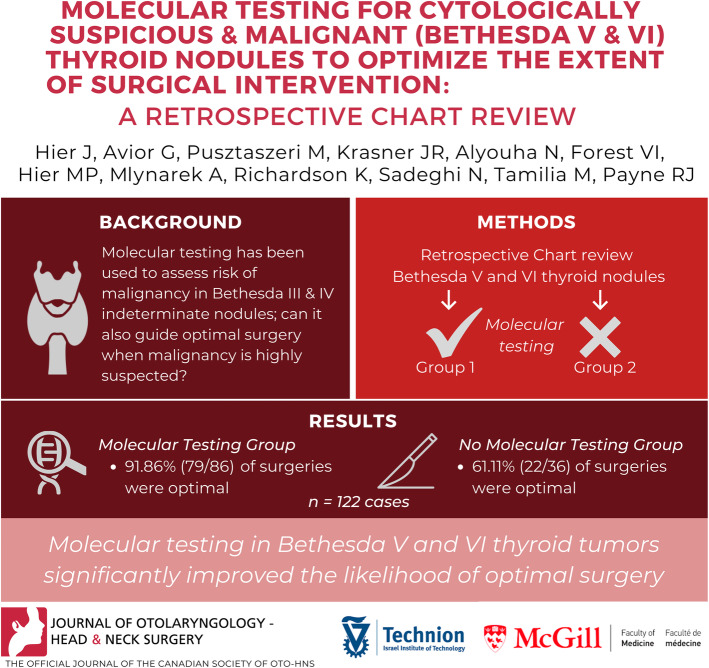
Molecular testing for cytologically suspicious and malignant (Bethesda V and VI) thyroid nodules to optimize the extent of surgical intervention: a retrospective chart review.
Jessica Hier, Galit Avior, Marc Pusztaszeri, Joshua R Krasner, Noura Alyouha, Veronique-Isabelle Forest, Michael P Hier, Alex Mlynarek, Keith Richardson, Nader Sadeghi, Michael Tamilia, Richard J Payne
{"title":"Molecular testing for cytologically suspicious and malignant (Bethesda V and VI) thyroid nodules to optimize the extent of surgical intervention: a retrospective chart review.","authors":"Jessica Hier, Galit Avior, Marc Pusztaszeri, Joshua R Krasner, Noura Alyouha, Veronique-Isabelle Forest, Michael P Hier, Alex Mlynarek, Keith Richardson, Nader Sadeghi, Michael Tamilia, Richard J Payne","doi":"10.1186/s40463-021-00500-6","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Molecular testing has been used for cytologically indeterminate thyroid nodules (Bethesda III and IV), where the risk of malignancy is 10-40%. However, to date, the role of molecular testing in cytologically suspicious or positive for malignancy (Bethesda V and VI) thyroid nodules has been controversial. The aim of this study was to determine whether patients who had molecular testing in Bethesda V and VI thyroid nodules had the optimal extent of surgery performed more often than patients who did not have molecular testing performed.</p><p><strong>Methods: </strong>A retrospective chart review of 122 cases was performed: 101 patients from the McGill University teaching hospitals and 21 patients from the Hillel Yaffe Medical center, Technion University. Patients included in the study were those with Bethesda V or VI thyroid nodules who underwent molecular testing (ThyGenext® or ThyroseqV3®) (McGill n = 72, Hillel Yaffe n = 14). Patients with Bethesda V or VI thyroid nodules who did not undergo molecular testing were used as controls (McGill n = 29, Hillel Yaffe n = 7). Each case was reviewed in order to determine whether the patient had optimal surgery. This was defined as total thyroidectomy in the presence of either a positive lymph node, extrathyroidal extension, or an aggressive pathological variant of papillary thyroid carcinoma (tall cell, hobnail, columnar cell, diffuse sclerosing, and solid/trabecular) documented on the final pathology report. In all other cases, a lobectomy/hemi/subtotal thyroidectomy was considered as optimal surgery. Chi-squared testing was performed to compare groups.</p><p><strong>Results: </strong>When molecular testing was done, 91.86% (79/86) of surgeries in the molecular testing group were optimal, compared to 61.11% (22/36) in the control group. At McGill University teaching hospitals and at Hillel Yaffe, 91.67% (66/72) and 92.86% (13/14) of surgeries in the intervention group were considered as optimal, respectively. This compares to 58.62% (17/29) at McGill and 71.43% (5/7) at Hillel Yaffe when molecular testing was not performed (p = .001, p = .186).</p><p><strong>Conclusions: </strong>In this study, molecular testing in Bethesda V and VI thyroid tumors significantly improved the likelihood of optimal surgery. Therefore, molecular testing may have an important role in optimizing surgical procedures performed in the setting of Bethesda V and VI thyroid nodules. Prospective studies with larger sample sizes are required to further investigate this finding.</p>","PeriodicalId":520683,"journal":{"name":"Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale","volume":" ","pages":"29"},"PeriodicalIF":2.2000,"publicationDate":"2021-04-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40463-021-00500-6","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of otolaryngology - head & neck surgery = Le Journal d'oto-rhino-laryngologie et de chirurgie cervico-faciale","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s40463-021-00500-6","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
Background: Molecular testing has been used for cytologically indeterminate thyroid nodules (Bethesda III and IV), where the risk of malignancy is 10-40%. However, to date, the role of molecular testing in cytologically suspicious or positive for malignancy (Bethesda V and VI) thyroid nodules has been controversial. The aim of this study was to determine whether patients who had molecular testing in Bethesda V and VI thyroid nodules had the optimal extent of surgery performed more often than patients who did not have molecular testing performed.
Methods: A retrospective chart review of 122 cases was performed: 101 patients from the McGill University teaching hospitals and 21 patients from the Hillel Yaffe Medical center, Technion University. Patients included in the study were those with Bethesda V or VI thyroid nodules who underwent molecular testing (ThyGenext® or ThyroseqV3®) (McGill n = 72, Hillel Yaffe n = 14). Patients with Bethesda V or VI thyroid nodules who did not undergo molecular testing were used as controls (McGill n = 29, Hillel Yaffe n = 7). Each case was reviewed in order to determine whether the patient had optimal surgery. This was defined as total thyroidectomy in the presence of either a positive lymph node, extrathyroidal extension, or an aggressive pathological variant of papillary thyroid carcinoma (tall cell, hobnail, columnar cell, diffuse sclerosing, and solid/trabecular) documented on the final pathology report. In all other cases, a lobectomy/hemi/subtotal thyroidectomy was considered as optimal surgery. Chi-squared testing was performed to compare groups.
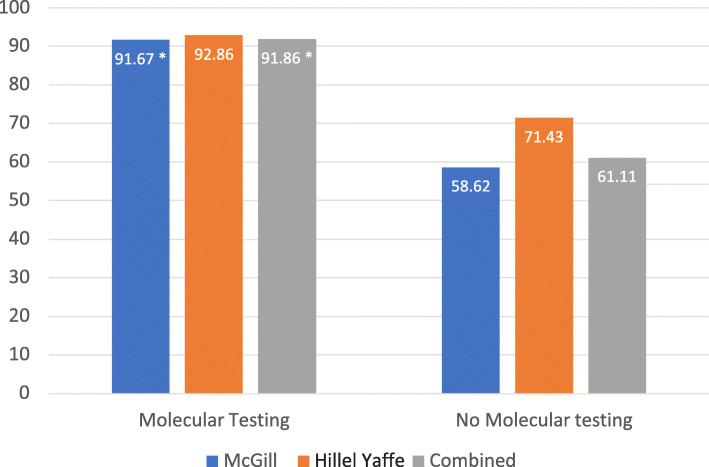
Results: When molecular testing was done, 91.86% (79/86) of surgeries in the molecular testing group were optimal, compared to 61.11% (22/36) in the control group. At McGill University teaching hospitals and at Hillel Yaffe, 91.67% (66/72) and 92.86% (13/14) of surgeries in the intervention group were considered as optimal, respectively. This compares to 58.62% (17/29) at McGill and 71.43% (5/7) at Hillel Yaffe when molecular testing was not performed (p = .001, p = .186).
Conclusions: In this study, molecular testing in Bethesda V and VI thyroid tumors significantly improved the likelihood of optimal surgery. Therefore, molecular testing may have an important role in optimizing surgical procedures performed in the setting of Bethesda V and VI thyroid nodules. Prospective studies with larger sample sizes are required to further investigate this finding.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


