Tomas J Saun, Jessica L Truong, Romy Ahluwalia, Robert R Richards
{"title":"A novel approach to the proximal interphalangeal joint: The volar oblique incision - a retrospective cohort study.","authors":"Tomas J Saun, Jessica L Truong, Romy Ahluwalia, Robert R Richards","doi":"10.1177/2059513120981941","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The surgical approach to the volar structures in the digits must be designed to provide adequate exposure of tendons, vessels and nerves but also in a way that prevents flexion contracture of the digit as the scar contracts. This is traditionally done using a zigzag 'Bruner' incision, first described by Dr Julian M Bruner in 1967. In this paper, we describe an alternative approach, the Volar Oblique incision, and present a single institutional cohort of patients who have undergone procedures beginning with this approach.</p><p><strong>Methods: </strong>A retrospective cohort study was performed on eight cases that involved a Bruner incision and eight similar cases that involved a volar oblique incision. Charts were reviewed for demographic data. Patients were asked to return to clinic postoperatively for scar assessment using the Patient and Observer Scar Assessment Scale (POSAS), where lower scores correspond to more favourable scar characteristics. The average follow-up period was 22 months. While in clinic, standard joint measurements were taken to assess for any proximal interphalangeal joint contracture. Demographics and questionnaire data were analysed using the Mann-Whitney U test for non-parametric data and quantitative joint measurements were analysed using Student's <i>t</i>-test.</p><p><strong>Results: </strong>There was no difference in flexion contracture between the two groups. The POSAS patient score for scar irregularity was lower in the volar oblique group compared to the Bruner group, but there was no difference in any of the other subcategories, the total patient score, nor the overall patient opinion. The total POSAS observer score was lower in the volar oblique group compared to the Bruner group, with lower scores in the scar thickness, observed relief and observed pliability subcategories as well as the overall observer opinion.</p><p><strong>Conclusion: </strong>The volar oblique incision appears to be satisfactory alternative to the classic Bruner incision in hand surgery that requires volar exposure of the digits. Future studies are needed to assess the validity of these findings on a larger scale.</p><p><strong>Lay summary: </strong>There are various types of incisions that surgeons use when they operate on fingers. When choosing an incision, it is important that the incision provides good exposure to the deeper structures but does not form a tight scar that limits movement of the finger (contracture).A commonly used incision for the palmar side of the finger is the zig-zag or 'Bruner' incision. Some people, however, find this zig-zag scar unappealing. We started using a single diagonal incision, which we have called the volar oblique, instead of the zig-zag Bruner for access to the middle joint of the finger. We wanted to describe the volar oblique technique and then compare the quality of these two scars and also assess if one limits movement of the finger more than the other.Our research found no differences in finger contracture between groups. We did, however, find that patients reported scar irregularity more favourably in the volar oblique group and that surgeons rated scar thickness, relief (roughness) and pliability of the volar oblique scar higher than that of the zig-zag Bruner scar.This research presents a novel surgical technique and compares its results with respect to scar quality and finger contracture to the more traditional zig-zag Bruner approach.</p>","PeriodicalId":21495,"journal":{"name":"Scars, burns & healing","volume":"6 ","pages":"2059513120981941"},"PeriodicalIF":0.0000,"publicationDate":"2020-12-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/75/67/10.1177_2059513120981941.PMC7780168.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Scars, burns & healing","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2059513120981941","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
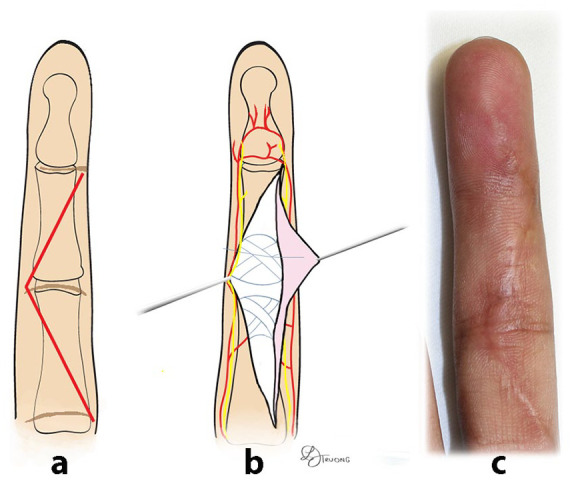
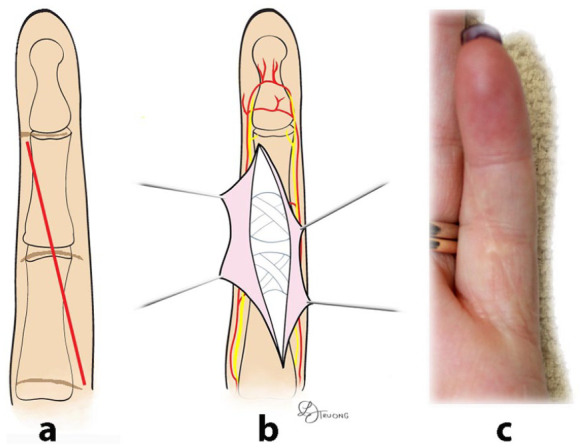
Background: The surgical approach to the volar structures in the digits must be designed to provide adequate exposure of tendons, vessels and nerves but also in a way that prevents flexion contracture of the digit as the scar contracts. This is traditionally done using a zigzag 'Bruner' incision, first described by Dr Julian M Bruner in 1967. In this paper, we describe an alternative approach, the Volar Oblique incision, and present a single institutional cohort of patients who have undergone procedures beginning with this approach.
Methods: A retrospective cohort study was performed on eight cases that involved a Bruner incision and eight similar cases that involved a volar oblique incision. Charts were reviewed for demographic data. Patients were asked to return to clinic postoperatively for scar assessment using the Patient and Observer Scar Assessment Scale (POSAS), where lower scores correspond to more favourable scar characteristics. The average follow-up period was 22 months. While in clinic, standard joint measurements were taken to assess for any proximal interphalangeal joint contracture. Demographics and questionnaire data were analysed using the Mann-Whitney U test for non-parametric data and quantitative joint measurements were analysed using Student's t-test.
Results: There was no difference in flexion contracture between the two groups. The POSAS patient score for scar irregularity was lower in the volar oblique group compared to the Bruner group, but there was no difference in any of the other subcategories, the total patient score, nor the overall patient opinion. The total POSAS observer score was lower in the volar oblique group compared to the Bruner group, with lower scores in the scar thickness, observed relief and observed pliability subcategories as well as the overall observer opinion.
Conclusion: The volar oblique incision appears to be satisfactory alternative to the classic Bruner incision in hand surgery that requires volar exposure of the digits. Future studies are needed to assess the validity of these findings on a larger scale.
Lay summary: There are various types of incisions that surgeons use when they operate on fingers. When choosing an incision, it is important that the incision provides good exposure to the deeper structures but does not form a tight scar that limits movement of the finger (contracture).A commonly used incision for the palmar side of the finger is the zig-zag or 'Bruner' incision. Some people, however, find this zig-zag scar unappealing. We started using a single diagonal incision, which we have called the volar oblique, instead of the zig-zag Bruner for access to the middle joint of the finger. We wanted to describe the volar oblique technique and then compare the quality of these two scars and also assess if one limits movement of the finger more than the other.Our research found no differences in finger contracture between groups. We did, however, find that patients reported scar irregularity more favourably in the volar oblique group and that surgeons rated scar thickness, relief (roughness) and pliability of the volar oblique scar higher than that of the zig-zag Bruner scar.This research presents a novel surgical technique and compares its results with respect to scar quality and finger contracture to the more traditional zig-zag Bruner approach.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


