Stephen J Wallace, Michael P Murphy, Corey J Schiffman, William J Hopkinson, Nicholas M Brown
{"title":"Demographic data is more predictive of component size than digital radiographic templating in total knee arthroplasty.","authors":"Stephen J Wallace, Michael P Murphy, Corey J Schiffman, William J Hopkinson, Nicholas M Brown","doi":"10.1186/s43019-020-00075-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Preoperative radiographic templating for total knee arthroplasty (TKA) has been shown to be inaccurate. Patient demographic data, such as gender, height, weight, age, and race, may be more predictive of implanted component size in TKA.</p><p><strong>Materials and methods: </strong>A multivariate linear regression model was designed to predict implanted femoral and tibial component size using demographic data along a consecutive series of 201 patients undergoing index TKA. Traditional, two-dimensional, radiographic templating was compared to demographic-based regression predictions on a prospective 181 consecutive patients undergoing index TKA in their ability to accurately predict intraoperative implanted sizes. Surgeons were blinded of any predictions.</p><p><strong>Results: </strong>Patient gender, height, weight, age, and ethnicity/race were predictive of implanted TKA component size. The regression model more accurately predicted implanted component size compared to radiographically templated sizes for both the femoral (P = 0.04) and tibial (P < 0.01) components. The regression model exactly predicted femoral and tibial component sizes in 43.7 and 43.7% of cases, was within one size 90.1 and 95.6% of the time, and was within two sizes in every case. Radiographic templating exactly predicted 35.4 and 36.5% of cases, was within one size 86.2 and 85.1% of the time, and varied up to four sizes for both the femoral and tibial components. The regression model averaged within 0.66 and 0.61 sizes, versus 0.81 and 0.81 sizes for radiographic templating for femoral and tibial components.</p><p><strong>Conclusions: </strong>A demographic-based regression model was created based on patient-specific demographic data to predict femoral and tibial TKA component sizes. In a prospective patient series, the regression model more accurately and precisely predicted implanted component sizes compared to radiographic templating.</p><p><strong>Level of evidence: </strong>Prospective cohort, level II.</p>","PeriodicalId":17886,"journal":{"name":"Knee Surgery & Related Research","volume":"32 1","pages":"63"},"PeriodicalIF":4.4000,"publicationDate":"2020-11-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s43019-020-00075-y","citationCount":"12","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Knee Surgery & Related Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s43019-020-00075-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 12
Abstract
Background: Preoperative radiographic templating for total knee arthroplasty (TKA) has been shown to be inaccurate. Patient demographic data, such as gender, height, weight, age, and race, may be more predictive of implanted component size in TKA.
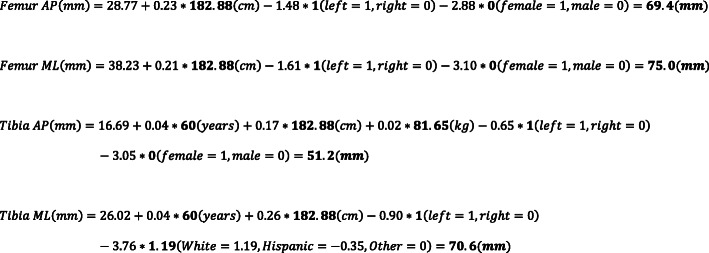
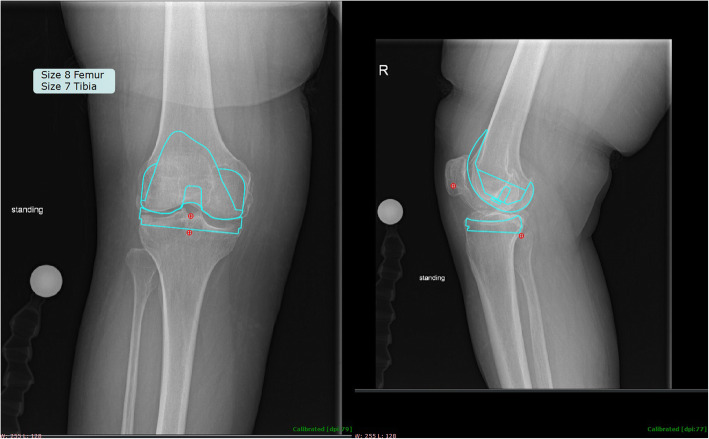
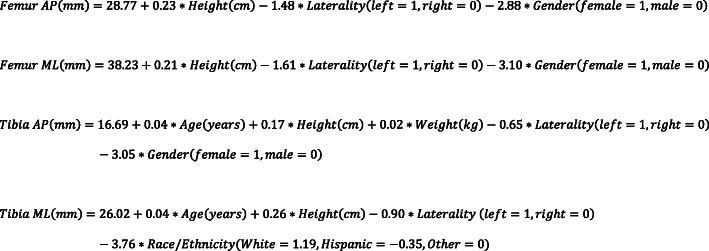
Materials and methods: A multivariate linear regression model was designed to predict implanted femoral and tibial component size using demographic data along a consecutive series of 201 patients undergoing index TKA. Traditional, two-dimensional, radiographic templating was compared to demographic-based regression predictions on a prospective 181 consecutive patients undergoing index TKA in their ability to accurately predict intraoperative implanted sizes. Surgeons were blinded of any predictions.
Results: Patient gender, height, weight, age, and ethnicity/race were predictive of implanted TKA component size. The regression model more accurately predicted implanted component size compared to radiographically templated sizes for both the femoral (P = 0.04) and tibial (P < 0.01) components. The regression model exactly predicted femoral and tibial component sizes in 43.7 and 43.7% of cases, was within one size 90.1 and 95.6% of the time, and was within two sizes in every case. Radiographic templating exactly predicted 35.4 and 36.5% of cases, was within one size 86.2 and 85.1% of the time, and varied up to four sizes for both the femoral and tibial components. The regression model averaged within 0.66 and 0.61 sizes, versus 0.81 and 0.81 sizes for radiographic templating for femoral and tibial components.
Conclusions: A demographic-based regression model was created based on patient-specific demographic data to predict femoral and tibial TKA component sizes. In a prospective patient series, the regression model more accurately and precisely predicted implanted component sizes compared to radiographic templating.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


