Peri-Procedural Blood Pressure Changes and Their Relationship with MACE in Patients Undergoing Percutaneous Coronary Intervention: A Cross-Sectional Study.
Susan Labib, Hussein Heshmat Kassem, Hossam Kandil
{"title":"Peri-Procedural Blood Pressure Changes and Their Relationship with MACE in Patients Undergoing Percutaneous Coronary Intervention: A Cross-Sectional Study.","authors":"Susan Labib, Hussein Heshmat Kassem, Hossam Kandil","doi":"10.2147/IBPC.S268848","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Peri-procedural blood-pressure (BP) changes were investigated and correlated to Major adverse cardiovascular events (MACE) as predictor of outcome for patients undergoing percutaneous coronary intervention (PCI); whether acute coronary syndrome (Unstable angina, or MI; STEMI or NSTEMI) or scheduled for elective PCI.</p><p><strong>Methods: </strong>Resting BP in the 204 recruited patients undergoing PCI throughout 2018 was measured thrice - in the ward before transferring to the cardiac catheterization lab (cath lab), in the cath lab, and after transfer to the recovery room. Patients were categorized based on their systolic and diastolic BP peri-procedural difference as systolic (SBP): with a large difference (>20 mmHg, n=47), with a small difference (≤20 mmHg, n=157) (shock patients excluded); diastolic (DBP): with a large difference (>10 mmHg, n=65), and with a small difference (≤10 mmHg, n=139). The primary end-points were MACE including all-cause mortality, non-fatal myocardial infarction, and stroke during the hospital stay. The Mann-Whitney U and Chi-square tests were used to analyze the data accordingly (p<0.005).</p><p><strong>Results: </strong>Within the category of MACE, cardiac mortality was the only adverse cardiac event encountered in the study sample. Cardiac mortality was significantly higher in both the large SBP-difference group versus the other group (10.6% vs 0.6%, p=0.003) and the large DBP-difference group versus the small-difference group (7.7% vs 0.7%, p=0.013).</p><p><strong>Conclusion: </strong>Peri-procedural systolic and diastolic BP differences, greater than 20 mmHg and 10 mmHg, respectively, correlated with MACE in all patients undergoing PCI.</p>","PeriodicalId":45299,"journal":{"name":"Integrated Blood Pressure Control","volume":"13 ","pages":"187-195"},"PeriodicalIF":2.7000,"publicationDate":"2020-12-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.2147/IBPC.S268848","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Integrated Blood Pressure Control","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/IBPC.S268848","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 1
Abstract
Background: Peri-procedural blood-pressure (BP) changes were investigated and correlated to Major adverse cardiovascular events (MACE) as predictor of outcome for patients undergoing percutaneous coronary intervention (PCI); whether acute coronary syndrome (Unstable angina, or MI; STEMI or NSTEMI) or scheduled for elective PCI.
Methods: Resting BP in the 204 recruited patients undergoing PCI throughout 2018 was measured thrice - in the ward before transferring to the cardiac catheterization lab (cath lab), in the cath lab, and after transfer to the recovery room. Patients were categorized based on their systolic and diastolic BP peri-procedural difference as systolic (SBP): with a large difference (>20 mmHg, n=47), with a small difference (≤20 mmHg, n=157) (shock patients excluded); diastolic (DBP): with a large difference (>10 mmHg, n=65), and with a small difference (≤10 mmHg, n=139). The primary end-points were MACE including all-cause mortality, non-fatal myocardial infarction, and stroke during the hospital stay. The Mann-Whitney U and Chi-square tests were used to analyze the data accordingly (p<0.005).
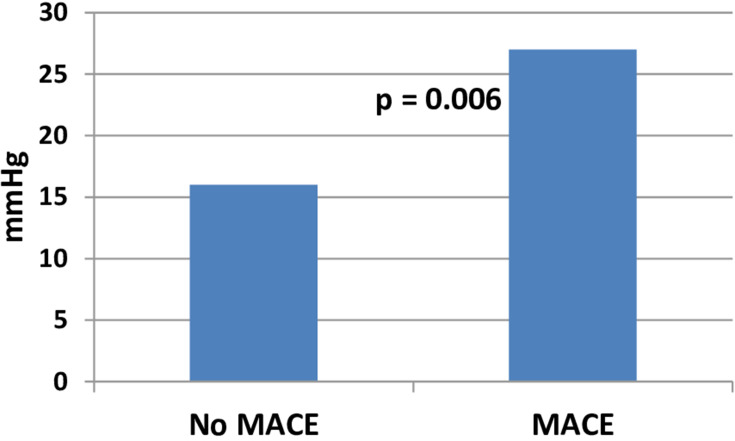
Results: Within the category of MACE, cardiac mortality was the only adverse cardiac event encountered in the study sample. Cardiac mortality was significantly higher in both the large SBP-difference group versus the other group (10.6% vs 0.6%, p=0.003) and the large DBP-difference group versus the small-difference group (7.7% vs 0.7%, p=0.013).
Conclusion: Peri-procedural systolic and diastolic BP differences, greater than 20 mmHg and 10 mmHg, respectively, correlated with MACE in all patients undergoing PCI.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


