Jennifer Chin, Bliss Kaneshiro, Jennifer Elia, Shandhini Raidoo, Michael Savala, Reni Soon
{"title":"Buffered lidocaine for paracervical blocks in first-trimester abortions: a randomized controlled trial","authors":"Jennifer Chin, Bliss Kaneshiro, Jennifer Elia, Shandhini Raidoo, Michael Savala, Reni Soon","doi":"10.1016/j.conx.2020.100044","DOIUrl":null,"url":null,"abstract":"<div><h3>Objective</h3><p>The objective was to evaluate if buffered lidocaine decreases injection pain as compared to plain lidocaine for paracervical blocks during first-trimester outpatient surgical abortions.</p></div><div><h3>Study design</h3><p>We conducted a randomized, double-blind, placebo-controlled trial among women undergoing outpatient uterine aspiration of a first-trimester pregnancy or an early pregnancy loss. Subjects received a paracervical block with either lidocaine 1% 20 mL or lidocaine 1% 18 mL plus sodium bicarbonate 8.4% 2 mL. The primary outcome was pain from injection of the paracervical block measured on a 100-mm visual analog scale (VAS). Secondary outcomes included pain after cervical dilation, uterine aspiration and overall satisfaction with pain control. Scores were compared using the Mann–Whitney <em>U</em> test. We aimed to detect a 15-mm difference in pain from injection of the paracervical block.</p></div><div><h3>Results</h3><p>From May 2017 to October 2018, 48 women received plain lidocaine and 50 women received buffered lidocaine. Groups were similar in demographics. We found no clinically or statistically meaningful difference in pain when evaluating median VAS scores for paracervical block injection between the buffered and plain lidocaine [30.0 (interquartile range (IQR) 15.3–64.5); 44.5 (IQR 18.3–65), respectively, p = .32]. We found no difference in secondary outcomes between buffered and plain lidocaine.</p></div><div><h3>Conclusion</h3><p>Buffered lidocaine for paracervical blocks in first-trimester outpatient surgical abortions does not decrease injection pain as compared to plain lidocaine.</p></div><div><h3>Implications statement</h3><p>Buffering the paracervical block in first-trimester outpatient surgical abortions does not decrease injection pain as compared to plain lidocaine, nor does it increase patient satisfaction. Eliminating sodium bicarbonate allows for a more cost-effective and readily available solution for paracervical blocks.</p></div>","PeriodicalId":10655,"journal":{"name":"Contraception: X","volume":"2 ","pages":"Article 100044"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1016/j.conx.2020.100044","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Contraception: X","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2590151620300277","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 1
Abstract
Objective
The objective was to evaluate if buffered lidocaine decreases injection pain as compared to plain lidocaine for paracervical blocks during first-trimester outpatient surgical abortions.
Study design
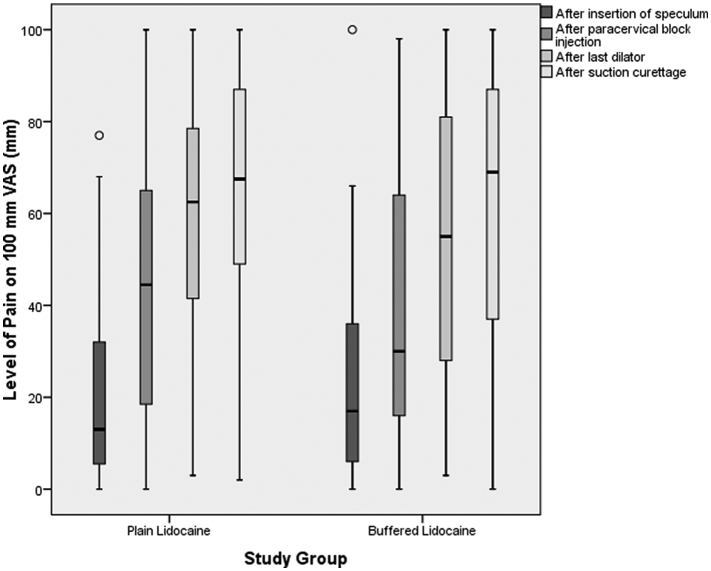
We conducted a randomized, double-blind, placebo-controlled trial among women undergoing outpatient uterine aspiration of a first-trimester pregnancy or an early pregnancy loss. Subjects received a paracervical block with either lidocaine 1% 20 mL or lidocaine 1% 18 mL plus sodium bicarbonate 8.4% 2 mL. The primary outcome was pain from injection of the paracervical block measured on a 100-mm visual analog scale (VAS). Secondary outcomes included pain after cervical dilation, uterine aspiration and overall satisfaction with pain control. Scores were compared using the Mann–Whitney U test. We aimed to detect a 15-mm difference in pain from injection of the paracervical block.
Results
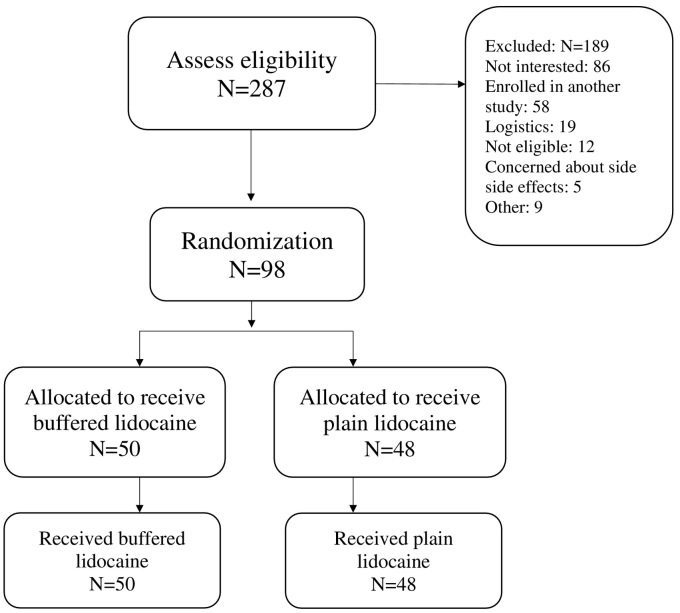
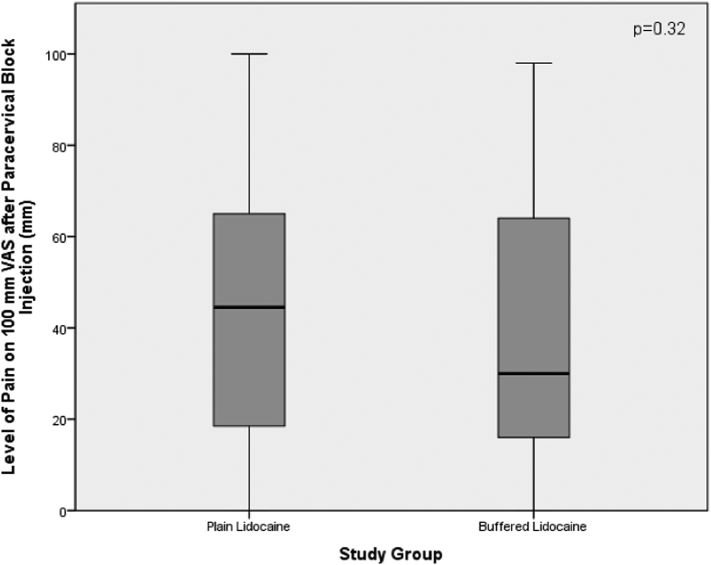
From May 2017 to October 2018, 48 women received plain lidocaine and 50 women received buffered lidocaine. Groups were similar in demographics. We found no clinically or statistically meaningful difference in pain when evaluating median VAS scores for paracervical block injection between the buffered and plain lidocaine [30.0 (interquartile range (IQR) 15.3–64.5); 44.5 (IQR 18.3–65), respectively, p = .32]. We found no difference in secondary outcomes between buffered and plain lidocaine.
Conclusion
Buffered lidocaine for paracervical blocks in first-trimester outpatient surgical abortions does not decrease injection pain as compared to plain lidocaine.
Implications statement
Buffering the paracervical block in first-trimester outpatient surgical abortions does not decrease injection pain as compared to plain lidocaine, nor does it increase patient satisfaction. Eliminating sodium bicarbonate allows for a more cost-effective and readily available solution for paracervical blocks.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


