{"title":"Paediatric formulations of artemisinin-based combination therapies for treating uncomplicated malaria in children.","authors":"Sabine Bélard, Michael Ramharter, Florian Kurth","doi":"10.1002/14651858.CD009568.pub2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>In endemic malarial areas, young children have high levels of malaria morbidity and mortality. The World Health Organization recommends oral artemisinin-based combination therapy (ACT) for treating uncomplicated malaria. Paediatric formulations of ACT have been developed to make it easier to treat children.</p><p><strong>Objectives: </strong>To evaluate evidence from trials on the efficacy, safety, tolerability, and acceptability of paediatric ACT formulations compared to tablet ACT formulations for uncomplicated P falciparum malaria in children up to 14 years old.</p><p><strong>Search methods: </strong>We searched the Cochrane Infectious Diseases Group Specialized Register; Cochrane Central Register of Controlled Trials (CENTRAL); MEDLINE; Embase; the Latin American and Caribbean Health Science Information database (LILACS); ISI Web of Science; Google Scholar; Scopus; and the metaRegister of Controlled Trials (mRCT) to 11 December 2019.</p><p><strong>Selection criteria: </strong>We included randomised controlled clinical trials (RCTs) of paediatric versus non-paediatric formulated ACT in children aged 14 years or younger with acute uncomplicated malaria.</p><p><strong>Data collection and analysis: </strong>Two authors independently assessed eligibility and risk of bias, and carried out data extraction. We analyzed the primary outcomes of efficacy, safety and tolerability of paediatric versus non-paediatric ACT using risk ratios (RR) and 95% confidence intervals (CI). Secondary outcomes were: treatment failure on the last day of observation (day 42), fever clearance time, parasite clearance time, pharmacokinetics, and acceptability.</p><p><strong>Main results: </strong>Three trials met the inclusion criteria. Two compared a paediatric dispersible tablet formulation against crushed tablets of artemether-lumefantrine (AL) and dihydroartemisinin-piperaquine (DHA-PQ), and one trial assessed artemether-lumefantrine formulated as powder for suspension compared with crushed tablets. The trials were carried out between 2006 and 2015 in sub-Saharan Africa (Benin, Mali, Mozambique, Tanzania, Kenya, Democratic Republic of the Congo, Burkina Faso, and The Gambia). In all three trials, the paediatric and control ACT achieved polymerase chain reaction (PCR)-adjusted treatment failure rates of < 10% on day 28 in the per-protocol (PP) population. For the comparison of dispersible versus crushed tablets, the two trials did not detect a difference for treatment failure by day 28 (PCR-adjusted PP population: RR 1.35, 95% CI 0.49 to 3.72; 1061 participants, 2 studies, low-certainty evidence). Similarly, for the comparison of suspension versus crushed tablet ACT, we did not detect any difference in treatment failure at day 28 (PCR-adjusted PP population: RR 1.64, 95% CI 0.55 to 4.87; 245 participants, 1 study). We did not detect any difference in serious adverse events for the comparison of dispersible versus crushed tablets (RR 1.05, 95% CI 0.38 to 2.88; 1197 participants, 2 studies, low-certainty evidence), or for the comparison of suspension versus crushed tablet ACT (RR 0.74, 95% CI 0.17 to 3.26; 267 participants, 1 study). In the dispersible ACT arms, drug-related adverse events occurred in 9% of children in the AL study and 34% of children in the DHA-PQ study. In the control arms, drug-related adverse events occurred in 12% of children in the AL study and in 42% of children in the DHA-PQ study. Drug-related adverse events were lower in the dispersible ACT arms (RR 0.78, 95% CI 0.62 to 0.99; 1197 participants, 2 studies, moderate-certainty evidence). There was no detected difference in the rate of drug-related adverse events for suspension ACT versus crushed tablet ACT (RR 0.66, 95% CI 0.33 to 1.32; 267 participants, 1 study). Drug-related vomiting appeared to be less common in the dispersible ACT arms (RR 0.75, 95% CI 0.56 to 1.01; 1197 participants, 2 studies, low-certainty evidence) and in the suspension ACT arm (RR 0.66, 95% CI 0.33 to 1.32; 267 participants, 1 study), but both analyses were underpowered. No study assessed acceptability.</p><p><strong>Authors' conclusions: </strong>Trials did not demonstrate a difference in efficacy between paediatric dispersible or suspension ACT when compared with the respective crushed tablet ACT for treating uncomplicated P falciparum malaria in children. However, the evidence is of low to moderate certainty due to limited power. There appeared to be fewer drug-related adverse events with dispersible ACT compared to crushed tablet ACT. None of the included studies assessed acceptability of paediatric ACT formulation.</p>","PeriodicalId":515753,"journal":{"name":"The Cochrane database of systematic reviews","volume":" ","pages":"CD009568"},"PeriodicalIF":0.0000,"publicationDate":"2020-12-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1002/14651858.CD009568.pub2","citationCount":"3","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Cochrane database of systematic reviews","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/14651858.CD009568.pub2","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 3
Abstract
Background: In endemic malarial areas, young children have high levels of malaria morbidity and mortality. The World Health Organization recommends oral artemisinin-based combination therapy (ACT) for treating uncomplicated malaria. Paediatric formulations of ACT have been developed to make it easier to treat children.
Objectives: To evaluate evidence from trials on the efficacy, safety, tolerability, and acceptability of paediatric ACT formulations compared to tablet ACT formulations for uncomplicated P falciparum malaria in children up to 14 years old.
Search methods: We searched the Cochrane Infectious Diseases Group Specialized Register; Cochrane Central Register of Controlled Trials (CENTRAL); MEDLINE; Embase; the Latin American and Caribbean Health Science Information database (LILACS); ISI Web of Science; Google Scholar; Scopus; and the metaRegister of Controlled Trials (mRCT) to 11 December 2019.
Selection criteria: We included randomised controlled clinical trials (RCTs) of paediatric versus non-paediatric formulated ACT in children aged 14 years or younger with acute uncomplicated malaria.
Data collection and analysis: Two authors independently assessed eligibility and risk of bias, and carried out data extraction. We analyzed the primary outcomes of efficacy, safety and tolerability of paediatric versus non-paediatric ACT using risk ratios (RR) and 95% confidence intervals (CI). Secondary outcomes were: treatment failure on the last day of observation (day 42), fever clearance time, parasite clearance time, pharmacokinetics, and acceptability.
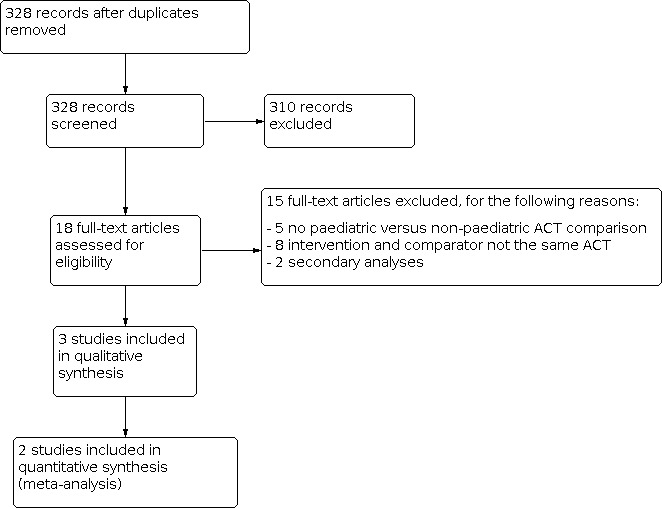
Main results: Three trials met the inclusion criteria. Two compared a paediatric dispersible tablet formulation against crushed tablets of artemether-lumefantrine (AL) and dihydroartemisinin-piperaquine (DHA-PQ), and one trial assessed artemether-lumefantrine formulated as powder for suspension compared with crushed tablets. The trials were carried out between 2006 and 2015 in sub-Saharan Africa (Benin, Mali, Mozambique, Tanzania, Kenya, Democratic Republic of the Congo, Burkina Faso, and The Gambia). In all three trials, the paediatric and control ACT achieved polymerase chain reaction (PCR)-adjusted treatment failure rates of < 10% on day 28 in the per-protocol (PP) population. For the comparison of dispersible versus crushed tablets, the two trials did not detect a difference for treatment failure by day 28 (PCR-adjusted PP population: RR 1.35, 95% CI 0.49 to 3.72; 1061 participants, 2 studies, low-certainty evidence). Similarly, for the comparison of suspension versus crushed tablet ACT, we did not detect any difference in treatment failure at day 28 (PCR-adjusted PP population: RR 1.64, 95% CI 0.55 to 4.87; 245 participants, 1 study). We did not detect any difference in serious adverse events for the comparison of dispersible versus crushed tablets (RR 1.05, 95% CI 0.38 to 2.88; 1197 participants, 2 studies, low-certainty evidence), or for the comparison of suspension versus crushed tablet ACT (RR 0.74, 95% CI 0.17 to 3.26; 267 participants, 1 study). In the dispersible ACT arms, drug-related adverse events occurred in 9% of children in the AL study and 34% of children in the DHA-PQ study. In the control arms, drug-related adverse events occurred in 12% of children in the AL study and in 42% of children in the DHA-PQ study. Drug-related adverse events were lower in the dispersible ACT arms (RR 0.78, 95% CI 0.62 to 0.99; 1197 participants, 2 studies, moderate-certainty evidence). There was no detected difference in the rate of drug-related adverse events for suspension ACT versus crushed tablet ACT (RR 0.66, 95% CI 0.33 to 1.32; 267 participants, 1 study). Drug-related vomiting appeared to be less common in the dispersible ACT arms (RR 0.75, 95% CI 0.56 to 1.01; 1197 participants, 2 studies, low-certainty evidence) and in the suspension ACT arm (RR 0.66, 95% CI 0.33 to 1.32; 267 participants, 1 study), but both analyses were underpowered. No study assessed acceptability.
Authors' conclusions: Trials did not demonstrate a difference in efficacy between paediatric dispersible or suspension ACT when compared with the respective crushed tablet ACT for treating uncomplicated P falciparum malaria in children. However, the evidence is of low to moderate certainty due to limited power. There appeared to be fewer drug-related adverse events with dispersible ACT compared to crushed tablet ACT. None of the included studies assessed acceptability of paediatric ACT formulation.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


