{"title":"Prognostic Impact of Delirium in Older People With/Without Dementia: A Retrospective Cohort Study in Taiwan.","authors":"C-K Liang, H-Y Chuang, F-Y Hsiao, M-Y Chou, T-Y Liu, C-C Yang, L-K Chen","doi":"10.1007/s12603-020-1459-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Objectives: </strong>To elucidate the hypothetically different interactions between delirium and post-discharge prognostic indicators in elderly hospital inpatients with versus without dementia.</p><p><strong>Design: </strong>Retrospective cohort study of claims data by Taiwan National Health Insurance beneficiaries between 2002-2013.</p><p><strong>Setting: </strong>Records of public hospital admissions in the Taiwan National Health Insurance Research database.</p><p><strong>Participants: </strong>Propensity-score matched subgroups of patients with delirium superimposed on dementia (n = 922) versus dementia alone (n = 922), delirium alone (n = 680) versus neither delirium nor dementia (n = 680).</p><p><strong>Measurements: </strong>Mortality, emergency department visits, readmissions, and psychotropic drug use, within 30, 180, and 365 days of discharge, were analyzed using multivariate proportional hazards or logistic regression analyses.</p><p><strong>Results: </strong>Delirium superimposed on dementia was not associated with increased post-discharge mortality, or emergency department visits, but significantly increased the risk of readmissions at 365-day follow-up (adjusted HR, 95% CI: 1.26, 1.01-1.56). However, delirium without dementia was significantly associated with increased post-discharge mortality, emergency department visits and readmissions at 180 days and 365 days (respective adjusted HRs: mortality, 1.63 and 1.79; adjusted ORs: emergency department visits, 1.89 and 1.81; readmissions, 1.47 and 1.53). Delirium in patients both with dementia and without, was associated with six-fold higher likelihood of in-hospital psychotropic drug use, and doubled post-discharge psychotropic drug usage.</p><p><strong>Conclusions: </strong>The obvious association between in-hospital delirium and worsened long-term prognosis, irrespective of dementia, raises awareness to warrants proactive and multimodal prevention and intervention strategies. Furthermore, the mechanisms about different influence of delirium for patients with/without dementia need to be further explored.</p>","PeriodicalId":501202,"journal":{"name":"The Journal of Nutrition, Health & Aging","volume":" ","pages":"951-958"},"PeriodicalIF":0.0000,"publicationDate":"2020-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12280676/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The Journal of Nutrition, Health & Aging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s12603-020-1459-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Objectives: To elucidate the hypothetically different interactions between delirium and post-discharge prognostic indicators in elderly hospital inpatients with versus without dementia.
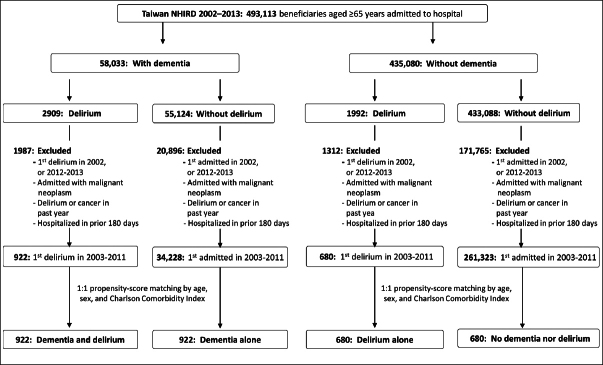
Design: Retrospective cohort study of claims data by Taiwan National Health Insurance beneficiaries between 2002-2013.
Setting: Records of public hospital admissions in the Taiwan National Health Insurance Research database.
Participants: Propensity-score matched subgroups of patients with delirium superimposed on dementia (n = 922) versus dementia alone (n = 922), delirium alone (n = 680) versus neither delirium nor dementia (n = 680).
Measurements: Mortality, emergency department visits, readmissions, and psychotropic drug use, within 30, 180, and 365 days of discharge, were analyzed using multivariate proportional hazards or logistic regression analyses.
Results: Delirium superimposed on dementia was not associated with increased post-discharge mortality, or emergency department visits, but significantly increased the risk of readmissions at 365-day follow-up (adjusted HR, 95% CI: 1.26, 1.01-1.56). However, delirium without dementia was significantly associated with increased post-discharge mortality, emergency department visits and readmissions at 180 days and 365 days (respective adjusted HRs: mortality, 1.63 and 1.79; adjusted ORs: emergency department visits, 1.89 and 1.81; readmissions, 1.47 and 1.53). Delirium in patients both with dementia and without, was associated with six-fold higher likelihood of in-hospital psychotropic drug use, and doubled post-discharge psychotropic drug usage.
Conclusions: The obvious association between in-hospital delirium and worsened long-term prognosis, irrespective of dementia, raises awareness to warrants proactive and multimodal prevention and intervention strategies. Furthermore, the mechanisms about different influence of delirium for patients with/without dementia need to be further explored.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


