{"title":"Prediction of pulmonary hypertension in older adults based on vital capacity and systolic pulmonary artery pressure.","authors":"Simon Wernhart, Jürgen Hedderich","doi":"10.1177/2048004020973834","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Right heart catheterization (RHC) is associated with a higher procedural risk in older adults, but non-invasive estimation of pulmonary hypertension (PH) is a challenge. We aimed to elaborate a non-invasive prediction model to estimate PH.</p><p><strong>Methods and design: </strong>We retrospectively analysed 134 older adults (70.0 years ±12.3; 44.9% males) who reported to our clinic with unclear dyspnea between 01/2015 and 01/2020 and had received RHC as a part of their diagnostic workup. Lung function testing, analysis of blood gas samples, 6 min walk distance and echocardiography were performed within 24 hours of RHC.</p><p><strong>Main outcome measures: </strong>In a stepwise statistical approach by using an in/exclusion algorithm (using the AIC criterion) we analysed non-invasive parameters to test their value in predicting PH (defined as mean pulmonary artery pressure, PA<sub>mean</sub>, >25mmHg). Discrimination capability of the final model was measured by the AUC (area under curve) from an ROC (receiver operating characteristics) analysis.</p><p><strong>Results: </strong>We yielded a sensitivity of 87.2% and a specificity of 62.5% in a combinatorial logistical model with systolic pulmonary artery pressure (sPAP) and forced vital capacity (VC<sub>max</sub>), the discrimination index was 86.7%. The odds ratios for an increase of 10 mmHg of sPAP were 2.99 (2.08-4.65) and 1.86 (1.11-3.21) for a 1 l decrease in VC<sub>max</sub>. On their own, VC<sub>max</sub> proved to be specific (83.3%), while sPAP was a sensitive (79.1%) predictor for PH.</p><p><strong>Conclusions: </strong>We provide a combinatorial model to predict PH from sPAP and VC<sub>max</sub> in older adults, which may help to avoid invasive procedures.</p>","PeriodicalId":30457,"journal":{"name":"JRSM Cardiovascular Disease","volume":" ","pages":"2048004020973834"},"PeriodicalIF":1.5000,"publicationDate":"2020-11-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2048004020973834","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JRSM Cardiovascular Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2048004020973834","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
引用次数: 2
Abstract
Objective: Right heart catheterization (RHC) is associated with a higher procedural risk in older adults, but non-invasive estimation of pulmonary hypertension (PH) is a challenge. We aimed to elaborate a non-invasive prediction model to estimate PH.
Methods and design: We retrospectively analysed 134 older adults (70.0 years ±12.3; 44.9% males) who reported to our clinic with unclear dyspnea between 01/2015 and 01/2020 and had received RHC as a part of their diagnostic workup. Lung function testing, analysis of blood gas samples, 6 min walk distance and echocardiography were performed within 24 hours of RHC.
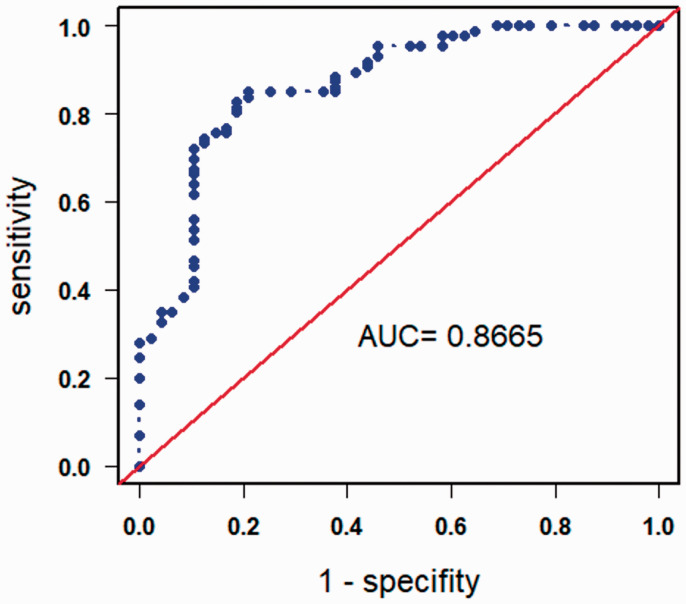
Main outcome measures: In a stepwise statistical approach by using an in/exclusion algorithm (using the AIC criterion) we analysed non-invasive parameters to test their value in predicting PH (defined as mean pulmonary artery pressure, PAmean, >25mmHg). Discrimination capability of the final model was measured by the AUC (area under curve) from an ROC (receiver operating characteristics) analysis.
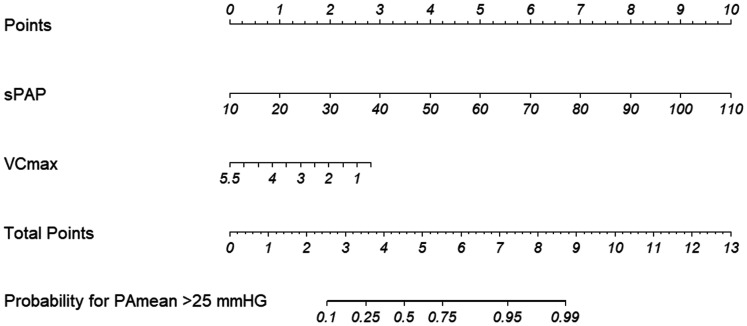
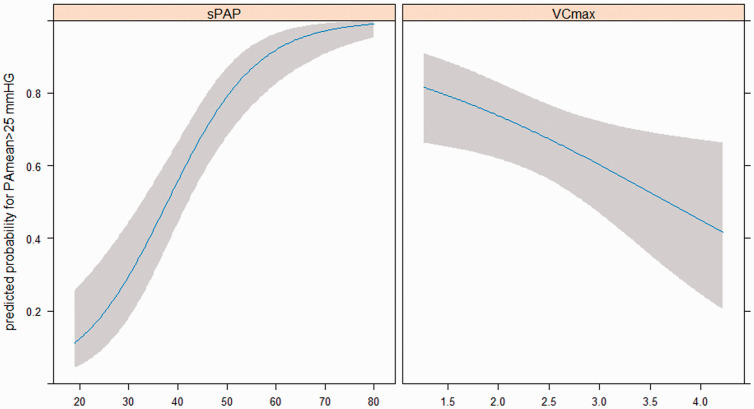
Results: We yielded a sensitivity of 87.2% and a specificity of 62.5% in a combinatorial logistical model with systolic pulmonary artery pressure (sPAP) and forced vital capacity (VCmax), the discrimination index was 86.7%. The odds ratios for an increase of 10 mmHg of sPAP were 2.99 (2.08-4.65) and 1.86 (1.11-3.21) for a 1 l decrease in VCmax. On their own, VCmax proved to be specific (83.3%), while sPAP was a sensitive (79.1%) predictor for PH.
Conclusions: We provide a combinatorial model to predict PH from sPAP and VCmax in older adults, which may help to avoid invasive procedures.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


