Chike John Okeke, Chukwudi Ogonnaya Okorie, Rufus Wale Ojewola, Njoku Isaac Omoke, Anselm Okwudili Obi, Agama Nnachi Egwu, Okechukwu Valentine Onyebum
{"title":"Delay of Surgery Start Time: Experience in a Nigerian Teaching Hospital.","authors":"Chike John Okeke, Chukwudi Ogonnaya Okorie, Rufus Wale Ojewola, Njoku Isaac Omoke, Anselm Okwudili Obi, Agama Nnachi Egwu, Okechukwu Valentine Onyebum","doi":"10.4103/njs.NJS_61_19","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Operating room delay has multiple negative effects on the patients, surgical team, and the hospital system. Maximum utilization of the operating room requires on-time knife on the skin and efficient turnover. Knowledge of the reasons for the delay will form a basis toward proffering solutions.</p><p><strong>Patients and methods: </strong>This was a prospective study of all consecutive elective cases done over a 15-month period from January 2016 to March 2017. Using our departmental protocol that \"knife on skin\" for the first elective case should be 8.00am, the delay was defined as a surgery starting later than 8.00am for the first cases while the interval between the cases of >30 min for the knife on the skin was used for subsequent cases. Reasons for delay in all cases of delay were documented. The prevalence and causes of the delays were analyzed. <i>P</i> < 0.05 was considered statistically significant.</p><p><strong>Results: </strong>Of 1178 surgeries performed during the period of study, 1170 (99.3%) of cases were delayed. The mean delay time was 151 min for all cases. First on the list had a longer delay time than others; 198.9 min versus 108.5 min (<i>P</i> = 0.000). Delay in the first cases accounted for 47.5% of all delayed cases. Overall, patient-related factor was the most common cause of delay (31.3%) followed in descending order by surgeon-related factor (28.5%) and hospital-related factor (26.2%). Patient-related factors accounted for 43.2% of first-case delays.</p><p><strong>Conclusion: </strong>Delays encountered in this study were multifactorial and are preventable. Efforts should be directed at these different causes of delay in the theater to mitigate these delays and improve productivity.</p>","PeriodicalId":30399,"journal":{"name":"Nigerian Journal of Surgery","volume":"26 2","pages":"110-116"},"PeriodicalIF":0.0000,"publicationDate":"2020-07-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6c/14/NJS-26-110.PMC7659763.pdf","citationCount":"2","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nigerian Journal of Surgery","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.4103/njs.NJS_61_19","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/7/27 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 2
Abstract
Background: Operating room delay has multiple negative effects on the patients, surgical team, and the hospital system. Maximum utilization of the operating room requires on-time knife on the skin and efficient turnover. Knowledge of the reasons for the delay will form a basis toward proffering solutions.
Patients and methods: This was a prospective study of all consecutive elective cases done over a 15-month period from January 2016 to March 2017. Using our departmental protocol that "knife on skin" for the first elective case should be 8.00am, the delay was defined as a surgery starting later than 8.00am for the first cases while the interval between the cases of >30 min for the knife on the skin was used for subsequent cases. Reasons for delay in all cases of delay were documented. The prevalence and causes of the delays were analyzed. P < 0.05 was considered statistically significant.
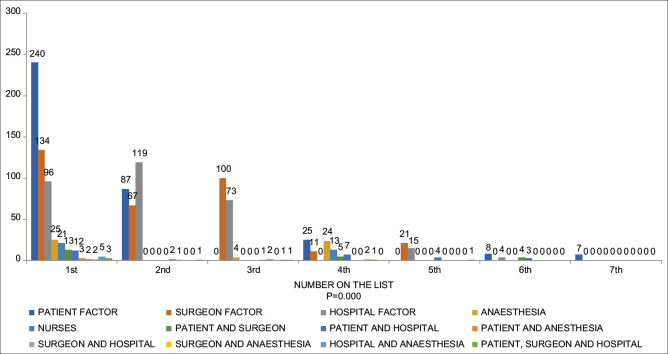
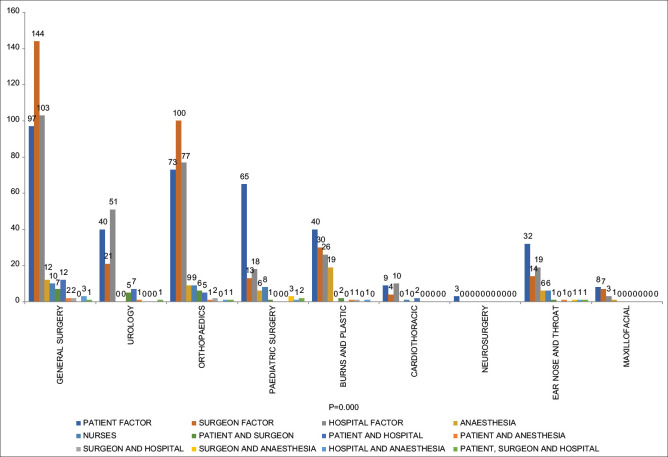
Results: Of 1178 surgeries performed during the period of study, 1170 (99.3%) of cases were delayed. The mean delay time was 151 min for all cases. First on the list had a longer delay time than others; 198.9 min versus 108.5 min (P = 0.000). Delay in the first cases accounted for 47.5% of all delayed cases. Overall, patient-related factor was the most common cause of delay (31.3%) followed in descending order by surgeon-related factor (28.5%) and hospital-related factor (26.2%). Patient-related factors accounted for 43.2% of first-case delays.
Conclusion: Delays encountered in this study were multifactorial and are preventable. Efforts should be directed at these different causes of delay in the theater to mitigate these delays and improve productivity.
背景:手术室延误对患者、手术团队和医院系统都有多重负面影响。最大限度地利用手术室,需要及时刀对皮肤和有效的周转。了解延迟的原因将成为提供解决方案的基础。患者和方法:这是一项前瞻性研究,在2016年1月至2017年3月的15个月内完成了所有连续的选择性病例。根据我们的科室方案,第一例选择性病例的“皮肤上刀”应在上午8点开始,延迟被定义为第一例病例的手术开始时间晚于上午8点,而后续病例的手术时间间隔大于30分钟。所有延误的原因都有文件记录。分析了延误的普遍性和原因。P < 0.05为差异有统计学意义。结果:研究期间共行1178例手术,延误1170例(99.3%)。所有病例的平均延迟时间为151 min。第一名的延迟时间比其他的要长;198.9 min vs 108.5 min (P = 0.000)。第一例延误占所有延误病例的47.5%。总体而言,患者相关因素是最常见的延迟原因(31.3%),其次是外科相关因素(28.5%)和医院相关因素(26.2%)。患者相关因素占首次病例延误的43.2%。结论:本研究中遇到的延误是多因素的,是可以预防的。应针对战区中造成延误的这些不同原因作出努力,以减轻这些延误并提高生产率。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


