Implementing a multilevel intervention to accelerate colorectal cancer screening and follow-up in federally qualified health centers using a stepped wedge design: a study protocol.
Karen Kim, Blasé Polite, Donald Hedeker, David Liebovitz, Fornessa Randal, Manasi Jayaprakash, Michael Quinn, Sang Mee Lee, Helen Lam
{"title":"Implementing a multilevel intervention to accelerate colorectal cancer screening and follow-up in federally qualified health centers using a stepped wedge design: a study protocol.","authors":"Karen Kim, Blasé Polite, Donald Hedeker, David Liebovitz, Fornessa Randal, Manasi Jayaprakash, Michael Quinn, Sang Mee Lee, Helen Lam","doi":"10.1186/s13012-020-01045-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Screening for colorectal cancer (CRC) not only detects disease early when treatment is more effective but also prevents cancer by finding and removing precancerous polyps. Because many of our nation's most disadvantaged and vulnerable individuals obtain health care at federally qualified health centers, these centers play a significant role in increasing CRC screening among the most vulnerable populations. Furthermore, the full benefits of cancer screenings must include timely and appropriate follow-up of abnormal results. Thus, the purpose of this study is to implement a multilevel intervention to increase rates of CRC screening, follow-up, and referral-to-care in federally qualified health centers, as well as simultaneously to observe and to gather information on the implementation process to improve the adoption, implementation, and sustainment of the intervention. The multilevel intervention will target three different levels of influences: organization, provider, and individual. It will have multiple components, including provider and staff education, provider reminder, provider assessment and feedback, patient reminder, and patient navigation.</p><p><strong>Methods: </strong>This study is a multilevel, three-phase, stepped wedge cluster randomized trial with four clusters of clinics from four different FQHC systems. In the first phase, there will be a 3-month waiting period during which no intervention components will be implemented. After the 3-month waiting period, we will randomize two clusters to cross from the control to the intervention and the remaining two clusters to follow 3 months later. All clusters will stay at the same phase for 9 months, followed by a 3-month transition period, and then cross over to the next phase.</p><p><strong>Discussion: </strong>There is a pressing need to reduce disparities in CRC outcomes, especially among racial/ethnic minority populations and among populations who live in poverty. Single-level interventions are often insufficient to lead to sustainable changes. Multilevel interventions, which target two or more levels of changes, are needed to address multilevel contextual influences simultaneously. Multilevel interventions with multiple components will affect not only the desired outcomes but also each other. How to take advantage of multilevel interventions and how to implement such interventions and evaluate their effectiveness are the ultimate goals of this study.</p><p><strong>Trial registration: </strong>This protocol is registered at clinicaltrials.gov ( NCT04514341 ) on 14 August 2020.</p>","PeriodicalId":417097,"journal":{"name":"Implementation Science : IS","volume":" ","pages":"96"},"PeriodicalIF":0.0000,"publicationDate":"2020-10-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s13012-020-01045-4","citationCount":"8","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Implementation Science : IS","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13012-020-01045-4","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 8
Abstract
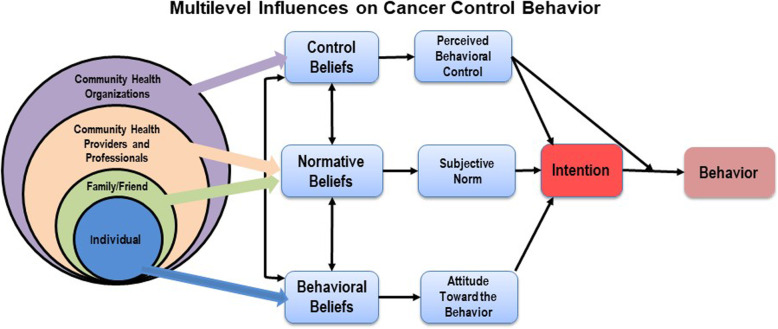
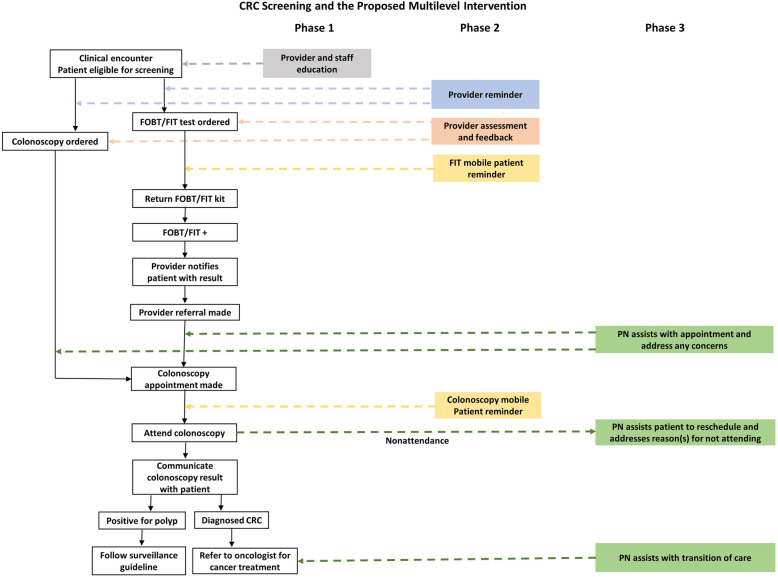
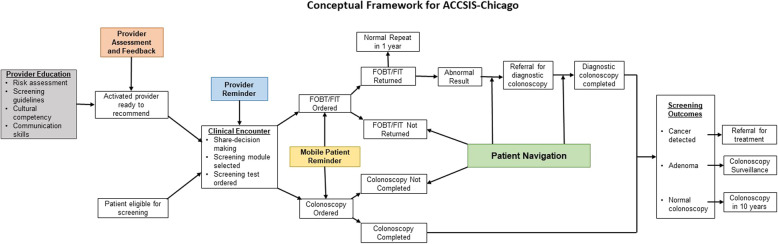
Background: Screening for colorectal cancer (CRC) not only detects disease early when treatment is more effective but also prevents cancer by finding and removing precancerous polyps. Because many of our nation's most disadvantaged and vulnerable individuals obtain health care at federally qualified health centers, these centers play a significant role in increasing CRC screening among the most vulnerable populations. Furthermore, the full benefits of cancer screenings must include timely and appropriate follow-up of abnormal results. Thus, the purpose of this study is to implement a multilevel intervention to increase rates of CRC screening, follow-up, and referral-to-care in federally qualified health centers, as well as simultaneously to observe and to gather information on the implementation process to improve the adoption, implementation, and sustainment of the intervention. The multilevel intervention will target three different levels of influences: organization, provider, and individual. It will have multiple components, including provider and staff education, provider reminder, provider assessment and feedback, patient reminder, and patient navigation.
Methods: This study is a multilevel, three-phase, stepped wedge cluster randomized trial with four clusters of clinics from four different FQHC systems. In the first phase, there will be a 3-month waiting period during which no intervention components will be implemented. After the 3-month waiting period, we will randomize two clusters to cross from the control to the intervention and the remaining two clusters to follow 3 months later. All clusters will stay at the same phase for 9 months, followed by a 3-month transition period, and then cross over to the next phase.
Discussion: There is a pressing need to reduce disparities in CRC outcomes, especially among racial/ethnic minority populations and among populations who live in poverty. Single-level interventions are often insufficient to lead to sustainable changes. Multilevel interventions, which target two or more levels of changes, are needed to address multilevel contextual influences simultaneously. Multilevel interventions with multiple components will affect not only the desired outcomes but also each other. How to take advantage of multilevel interventions and how to implement such interventions and evaluate their effectiveness are the ultimate goals of this study.
Trial registration: This protocol is registered at clinicaltrials.gov ( NCT04514341 ) on 14 August 2020.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


