Safety and efficacy of double vs. triple antithrombotic therapy in patients with atrial fibrillation with or without acute coronary syndrome undergoing percutaneous coronary intervention: a collaborative meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials.
Giuseppe Gargiulo, Christopher P Cannon, Charles Michael Gibson, Andreas Goette, Renato D Lopes, Jonas Oldgren, Serge Korjian, Stephan Windecker, Giovanni Esposito, Pascal Vranckx, Marco Valgimigli
{"title":"Safety and efficacy of double vs. triple antithrombotic therapy in patients with atrial fibrillation with or without acute coronary syndrome undergoing percutaneous coronary intervention: a collaborative meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials.","authors":"Giuseppe Gargiulo, Christopher P Cannon, Charles Michael Gibson, Andreas Goette, Renato D Lopes, Jonas Oldgren, Serge Korjian, Stephan Windecker, Giovanni Esposito, Pascal Vranckx, Marco Valgimigli","doi":"10.1093/ehjcvp/pvaa116","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Safety and efficacy of antithrombotic regimens in patients with atrial fibrillation (AF) undergoing percutaneous coronary intervention (PCI) may differ based on clinical presentation. We sought to compare double vs. triple antithrombotic therapy (DAT vs. TAT) in AF patients with or without acute coronary syndrome (ACS) undergoing PCI.</p><p><strong>Methods and results: </strong>A systematic review and meta-analysis was performed using PubMed to search for non-vitamin K antagonist oral anticoagulant (NOAC)-based randomized clinical trials. Data on subgroups of ACS or elective PCI were obtained by published reports or trial investigators. A total of 10 193 patients from four NOAC trials were analysed, of whom 5675 presenting with ACS (DAT = 3063 vs. TAT = 2612) and 4518 with stable coronary artery disease (SCAD; DAT = 2421 vs. TAT = 2097). The primary safety endpoint of ISTH major bleeding or clinically relevant non-major bleeding was reduced with DAT compared with TAT in both ACS (12.2% vs. 19.4%; RR 0.63, 95% CI 0.56-0.71; P < 0.0001; I2 = 0%) and SCAD (14.6% vs. 22.0%; RR 0.68, 95% CI 0.55-0.85; P = 0.0008; I2 = 66%), without interaction (P-int = 0.54). Findings were consistent for secondary bleeding endpoints, including intra-cranial haemorrhage. In both subgroups, there was no difference between DAT and TAT for all-cause death, major adverse cardiovascular events, or stroke. Myocardial infarction and stent thrombosis were numerically higher with DAT vs. TAT consistently in ACS and SCAD (P-int = 0.60 and 0.86, respectively). Findings were confirmed by multiple sensitivity analyses, including a separate analysis on dabigatran regimens and a restriction to PCI population.</p><p><strong>Conclusions: </strong>DAT, compared with TAT, is associated with lower bleeding risks, including intra-cranial haemorrhage, and a small non-significant excess of cardiac ischaemic events in both patients with or without ACS.</p>","PeriodicalId":11995,"journal":{"name":"European Heart Journal — Cardiovascular Pharmacotherapy","volume":" ","pages":"f50-f60"},"PeriodicalIF":0.0000,"publicationDate":"2021-04-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1093/ehjcvp/pvaa116","citationCount":"13","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal — Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvaa116","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 13
Abstract
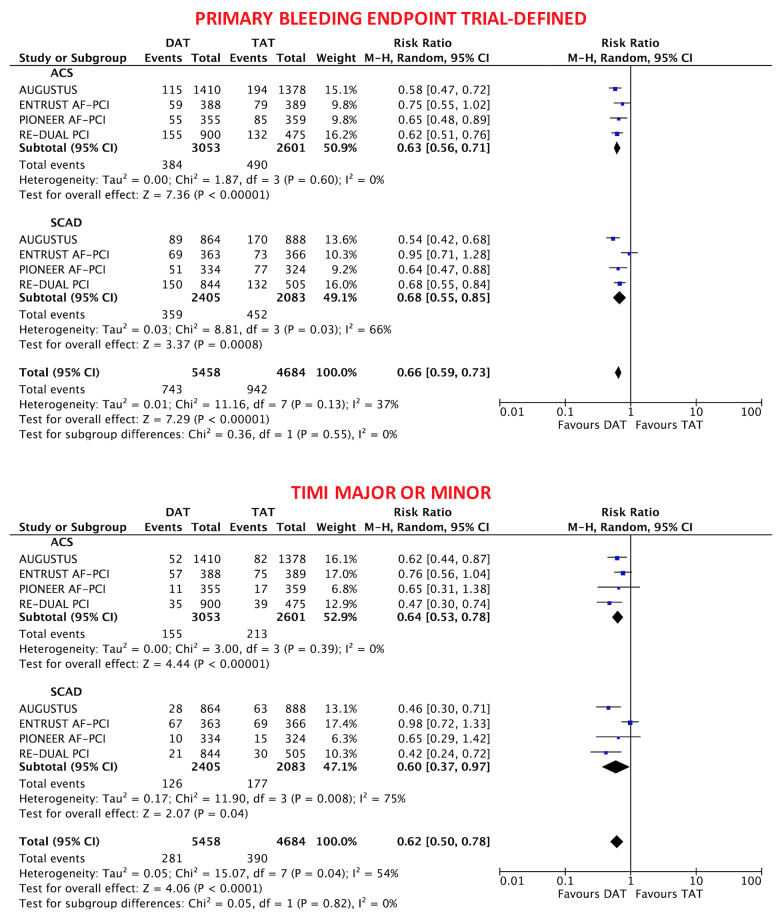
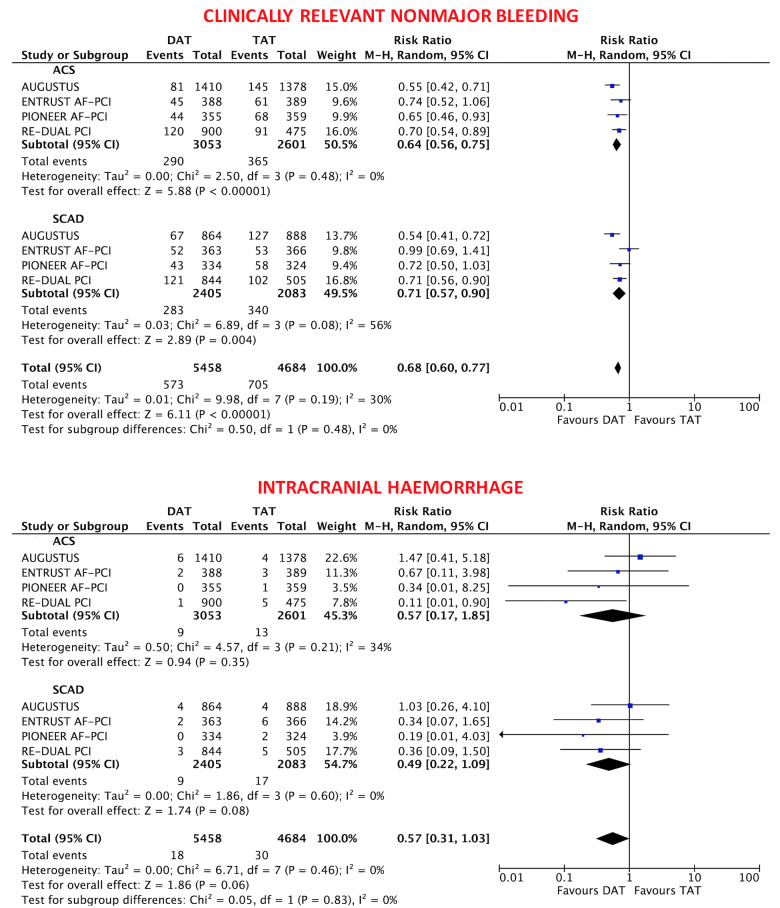
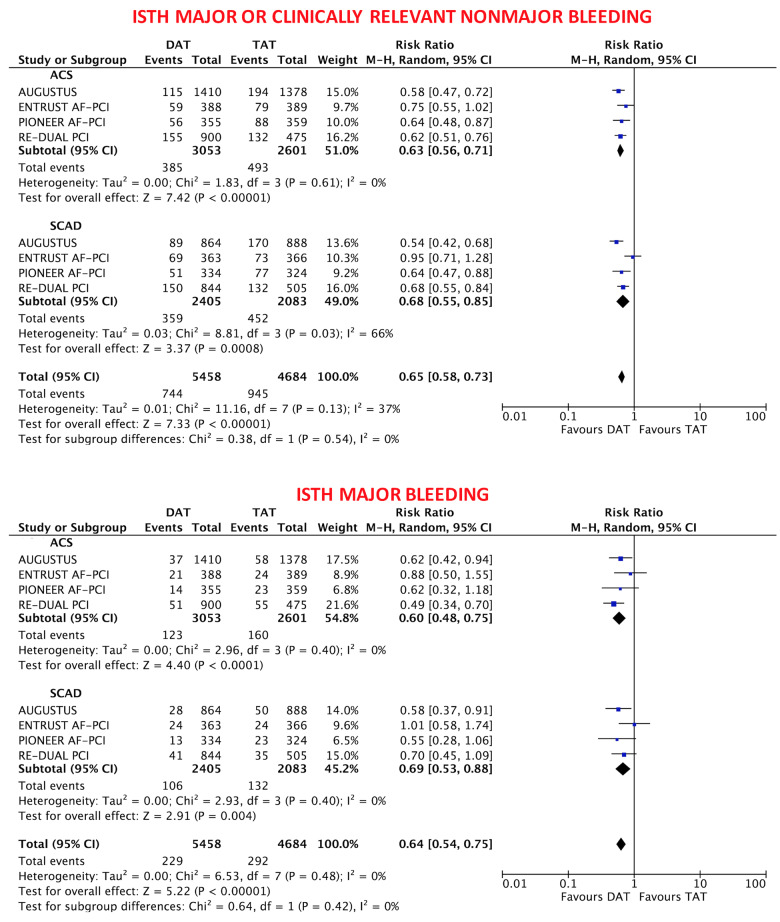
Aims: Safety and efficacy of antithrombotic regimens in patients with atrial fibrillation (AF) undergoing percutaneous coronary intervention (PCI) may differ based on clinical presentation. We sought to compare double vs. triple antithrombotic therapy (DAT vs. TAT) in AF patients with or without acute coronary syndrome (ACS) undergoing PCI.
Methods and results: A systematic review and meta-analysis was performed using PubMed to search for non-vitamin K antagonist oral anticoagulant (NOAC)-based randomized clinical trials. Data on subgroups of ACS or elective PCI were obtained by published reports or trial investigators. A total of 10 193 patients from four NOAC trials were analysed, of whom 5675 presenting with ACS (DAT = 3063 vs. TAT = 2612) and 4518 with stable coronary artery disease (SCAD; DAT = 2421 vs. TAT = 2097). The primary safety endpoint of ISTH major bleeding or clinically relevant non-major bleeding was reduced with DAT compared with TAT in both ACS (12.2% vs. 19.4%; RR 0.63, 95% CI 0.56-0.71; P < 0.0001; I2 = 0%) and SCAD (14.6% vs. 22.0%; RR 0.68, 95% CI 0.55-0.85; P = 0.0008; I2 = 66%), without interaction (P-int = 0.54). Findings were consistent for secondary bleeding endpoints, including intra-cranial haemorrhage. In both subgroups, there was no difference between DAT and TAT for all-cause death, major adverse cardiovascular events, or stroke. Myocardial infarction and stent thrombosis were numerically higher with DAT vs. TAT consistently in ACS and SCAD (P-int = 0.60 and 0.86, respectively). Findings were confirmed by multiple sensitivity analyses, including a separate analysis on dabigatran regimens and a restriction to PCI population.
Conclusions: DAT, compared with TAT, is associated with lower bleeding risks, including intra-cranial haemorrhage, and a small non-significant excess of cardiac ischaemic events in both patients with or without ACS.
目的:房颤(AF)经皮冠状动脉介入治疗(PCI)患者抗血栓治疗方案的安全性和有效性可能因临床表现而异。我们试图比较有或无急性冠脉综合征(ACS)的房颤患者行PCI的双重和三重抗血栓治疗(DAT和TAT)。方法和结果:通过PubMed进行系统回顾和荟萃分析,寻找基于非维生素K拮抗剂口服抗凝剂(NOAC)的随机临床试验。ACS亚组或选择性PCI的数据由已发表的报告或试验研究者获得。共分析了4项NOAC试验的10193例患者,其中5675例为ACS (DAT = 3063 vs. TAT = 2612), 4518例为稳定冠状动脉疾病(SCAD;DAT = 2421 vs. TAT = 2097)。在两种ACS中,与TAT相比,DAT降低了ISTH大出血或临床相关非大出血的主要安全终点(12.2% vs. 19.4%;Rr 0.63, 95% ci 0.56-0.71;结论:与TAT相比,DAT与较低的出血风险相关,包括颅内出血,以及伴有或不伴有ACS的心脏缺血事件的少量非显著性过量。

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


