IgA vasculitis with nephritis in cirrhotic Wilson disease: Is there an association?
Clinical Nephrology. Case Studies
Pub Date : 2020-10-12
eCollection Date: 2020-01-01
DOI:10.5414/CNCS110268
引用次数: 4
Abstract
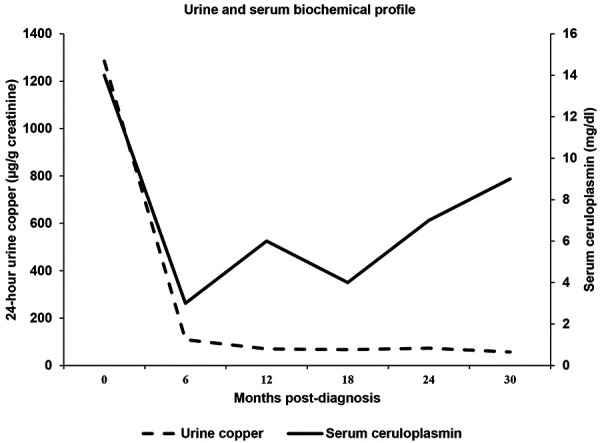
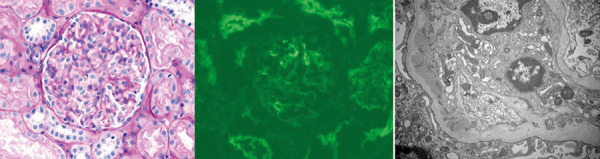
Introduction: IgA vasculitis (IgA-V) predominantly involves skin, gastrointestinal (GI) tract, joints, and kidneys. Wilson disease (WD) is a hepatolenticular degenerative disease caused by ATP7B gene mutation. Case report: Here we describe an unusual association of IgA-V with nephritis (IgA-VN) in an 11-year-old child with WD. He presented with palpable purpura without arthritis and GI involvement. Renal function was normal. Urinalysis showed microscopic hematuria and tubular proteinuria. Evaluation showed transaminitis, hypoalbuminemia, IgA hyperglobulinemia, and coagulation abnormalities. Serum ceruloplasmin and copper were low and 24-hour urine copper was extremely elevated. Liver biopsy showed stage IV cirrhosis with increased quantitative liver copper content. Skin and renal biopsy showed IgA-positive leukocytoclastic vasculitis and mesangial hyperplasia with IgA deposition, respectively. Quantitative renal copper content was normal. Homozygous pathogenic variant c.3207C>A (p.His1069Gln) of ATP7B was detected. There were no Kayser-Fleischer rings in the eyes, and neuropsychiatric examination was normal. Treatment with zinc and trientine led to normalization of hepatic function and serum IgA level with resolution of the rash and maintenance of renal function. Conclusion: Defective hepatic processing and/or clearance of IgA/IgA immune complexes probably led to the IgA-mediated skin and renal injury. Further such reports will help augment our understanding on the pathophysiology of IgA-VN in WD.
肝硬化Wilson病IgA血管炎伴肾炎:两者有关联吗?
简介:IgA血管炎(IgA- v)主要累及皮肤、胃肠道、关节和肾脏。肝豆状核变性(WD)是一种由ATP7B基因突变引起的肝豆状核变性疾病。病例报告:这里我们描述了一个罕见的IgA-V与肾炎(IgA-VN)的关联在11岁的儿童与WD。他表现为可触及的紫癜,没有关节炎和胃肠道受累。肾功能正常。尿检显示显微镜下血尿和管状蛋白尿。评估显示转氨炎、低白蛋白血症、IgA高球蛋白血症和凝血异常。血清铜蓝蛋白和铜含量低,24小时尿铜含量极高。肝活检显示IV期肝硬化,定量肝铜含量增高。皮肤和肾脏活检分别显示IgA阳性白细胞破壁性血管炎和系膜增生伴IgA沉积。肾铜定量含量正常。检测到ATP7B纯合子致病变异c.3207C>A (p.His1069Gln)。眼部无Kayser-Fleischer环,神经精神检查正常。锌和曲恩汀治疗导致肝功能和血清IgA水平正常化,皮疹消退,肾功能维持。结论:肝脏加工和/或清除IgA/IgA免疫复合物的缺陷可能导致IgA介导的皮肤和肾脏损伤。进一步的报道将有助于加深我们对IgA-VN在WD中的病理生理学的理解。
本文章由计算机程序翻译,如有差异,请以英文原文为准。
求助全文
约1分钟内获得全文
求助全文

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


