Modibo Sangare, Fatoumata Doumbia, Oumar Sidibe, Aboucacar Alassane Oumar, Sekou Bah, Modibo Kouyate, Seidina S Diakite, Karim Traore, Adama Karembe, Mohamed S Haidara, Souleymane P Coulibaly, Souleymane Coulibaly, Arouna Togora, Housseini Dolo, Drissa Traore, Seydou Doumbia, Mahamadou Diakite, Youssoufa Maiga, Amadou Diawara, Callixte Kuate, Hyung-Goo Kim, Gordon A Awandare
{"title":"Epilepsy Research in Mali: A Pilot Pharmacokinetics Study on First-Line Antiepileptic Drug Treatment.","authors":"Modibo Sangare, Fatoumata Doumbia, Oumar Sidibe, Aboucacar Alassane Oumar, Sekou Bah, Modibo Kouyate, Seidina S Diakite, Karim Traore, Adama Karembe, Mohamed S Haidara, Souleymane P Coulibaly, Souleymane Coulibaly, Arouna Togora, Housseini Dolo, Drissa Traore, Seydou Doumbia, Mahamadou Diakite, Youssoufa Maiga, Amadou Diawara, Callixte Kuate, Hyung-Goo Kim, Gordon A Awandare","doi":"10.14581/jer.20006","DOIUrl":null,"url":null,"abstract":"<p><strong>Background and purpose: </strong>The indication and benefit of plasma level of antiepileptic (AEDs) has been debating in the monitoring of people living with epilepsy and the epilepsy treatment gap has largely been documented in developed countries. This study was aimed to highlight the epilepsy treatment gap between rural and urban Mali.</p><p><strong>Methods: </strong>We conducted a pilot study on AEDs treatment from September 2016 to May 2019. For 6 months, 120 children and young adults living with epilepsy (rural site, 90; urban site, 30) received phenobarbital, valproic acid and/or carbamazepine. At our rural study site, we determined the AED plasma levels, monitored the frequency, severity and the duration of seizure, and administered monthly the McGill quality of life questionnaire. At our urban study site, each patient underwent an electroencephalogram and brain computed tomography scan without close monitoring.</p><p><strong>Results: </strong>At the rural study site, patients were mostly on monotherapy; AED levels at 1 month (M1) (n=90) and at 3 months (M3) (n=27) after inclusion were normal in 50% at M1 versus 55.6% at M3, low in 42.2% at M1 versus 33.3% at M3 and high in 7.8% at M1 versus 11.1% at M3. AED levels at M1 and at M3 were significantly different <i>p</i><0.0001. By M3, seizures (n=90) were <1/month in 26.7%, and lasted less than 1 minute in 16.7%. After a yearlong follow up, all 90 patients reported a good or excellent quality of life. At our urban study site, patients (n=30) were on carbamazepine and valproid acid in 66.67% and monotherapy (carbamazepine) in 33.33%. By November 2018, only six out 30 patients (on bi-therapy) were still taking their medications.</p><p><strong>Conclusions: </strong>Epilepsy diagnostic and treatment are a real concern in Mali. Our data showed appropriate AED treatment with close follow up resulted in a better quality of life of patients in rural Mali. We will promote the approach of personalized medicine in AED treatment in Mali.</p>","PeriodicalId":73741,"journal":{"name":"Journal of epilepsy research","volume":"10 1","pages":"31-39"},"PeriodicalIF":0.0000,"publicationDate":"2020-06-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://ftp.ncbi.nlm.nih.gov/pub/pmc/oa_pdf/6e/c1/jer-20006.PMC7494886.pdf","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of epilepsy research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14581/jer.20006","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/6/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background and purpose: The indication and benefit of plasma level of antiepileptic (AEDs) has been debating in the monitoring of people living with epilepsy and the epilepsy treatment gap has largely been documented in developed countries. This study was aimed to highlight the epilepsy treatment gap between rural and urban Mali.
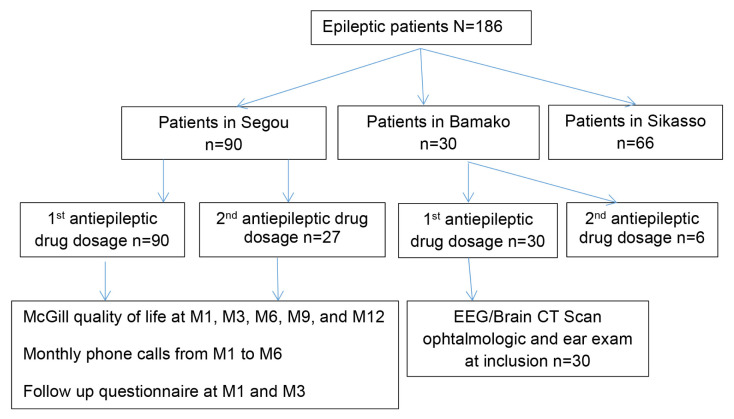
Methods: We conducted a pilot study on AEDs treatment from September 2016 to May 2019. For 6 months, 120 children and young adults living with epilepsy (rural site, 90; urban site, 30) received phenobarbital, valproic acid and/or carbamazepine. At our rural study site, we determined the AED plasma levels, monitored the frequency, severity and the duration of seizure, and administered monthly the McGill quality of life questionnaire. At our urban study site, each patient underwent an electroencephalogram and brain computed tomography scan without close monitoring.
Results: At the rural study site, patients were mostly on monotherapy; AED levels at 1 month (M1) (n=90) and at 3 months (M3) (n=27) after inclusion were normal in 50% at M1 versus 55.6% at M3, low in 42.2% at M1 versus 33.3% at M3 and high in 7.8% at M1 versus 11.1% at M3. AED levels at M1 and at M3 were significantly different p<0.0001. By M3, seizures (n=90) were <1/month in 26.7%, and lasted less than 1 minute in 16.7%. After a yearlong follow up, all 90 patients reported a good or excellent quality of life. At our urban study site, patients (n=30) were on carbamazepine and valproid acid in 66.67% and monotherapy (carbamazepine) in 33.33%. By November 2018, only six out 30 patients (on bi-therapy) were still taking their medications.
Conclusions: Epilepsy diagnostic and treatment are a real concern in Mali. Our data showed appropriate AED treatment with close follow up resulted in a better quality of life of patients in rural Mali. We will promote the approach of personalized medicine in AED treatment in Mali.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


