Matthias Hunger, Jennifer Eriksson, Stephane A Regnier, Katsuya Mori, John A Spertus, Joaquim Cristino
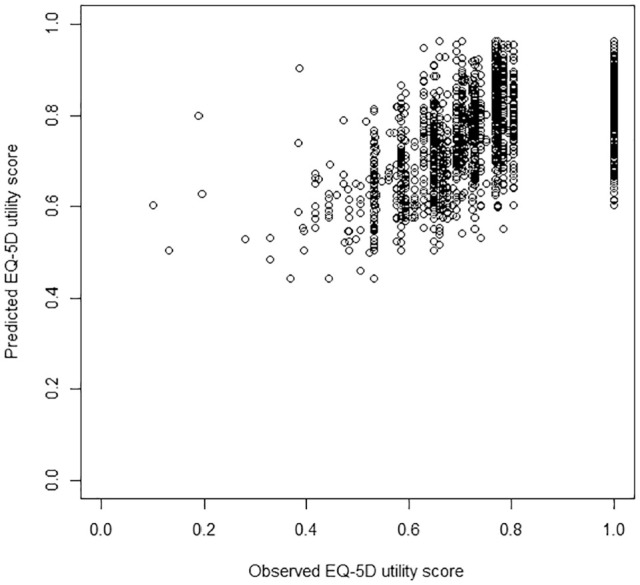
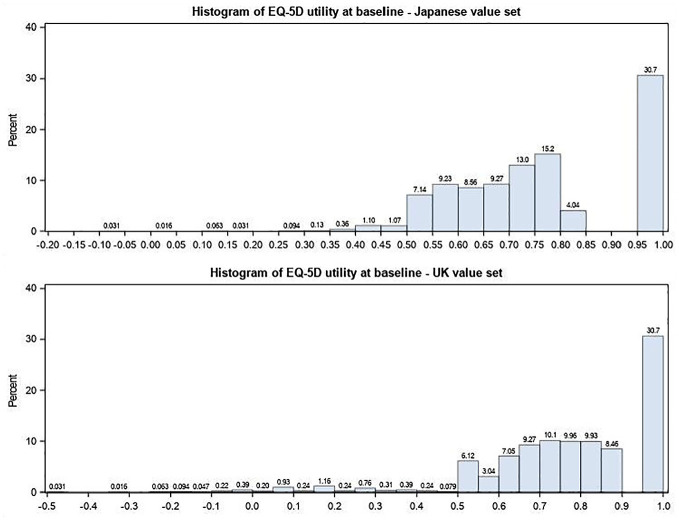
{"title":"Mapping the Kansas City Cardiomyopathy Questionnaire (KCCQ) Onto EQ-5D-3L in Heart Failure Patients: Results for the Japanese and UK Value Sets.","authors":"Matthias Hunger, Jennifer Eriksson, Stephane A Regnier, Katsuya Mori, John A Spertus, Joaquim Cristino","doi":"10.1177/2381468320971606","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background.</b> Health technology assessment bodies in several countries, including Japan and the United Kingdom, recommend mapping techniques to obtain utility scores in clinical trials that do not have a preference-based measure of health. This study sought to develop mapping algorithms to predict EQ-5D-3L scores from the Kansas City Cardiomyopathy Questionnaire (KCCQ) in patients with heart failure (HF). <b>Methods.</b> Data from the randomized, double-blind PARADIGM-HF trial were analyzed, and EQ-5D-3L scores were calculated using the Japanese and UK value sets. Several different model specifications were explored to best fit EQ-5D data collected at baseline with KCCQ scores, including ordinary least square regression, two-part, Tobit, and three-part models. Generalized estimating equations models were also fitted to analyze longitudinal EQ-5D data. To validate model predictions, the data set was split into a derivation (<i>n</i> = 4,465) from which the models were developed and a separate sample (<i>n</i> = 1,892) for validation. <b>Results.</b> There were only small differences between the different model classes tested. Model performance and predictive power was better for the item-level models than for the models including KCCQ domain scores. <i>R</i> <sup>2</sup> statistics for the item-level models ranged from 0.45 to 0.52. Mean absolute error in the validation sample was 0.10 for the models using the Japanese value set and 0.114 for the UK models. All models showed some underprediction of utility above 0.75 and overprediction of utility below 0.5, but performed well for population-level estimates. <b>Conclusions.</b> Using data from a large clinical trial in HF, we found that EQ-5D-3L scores can be estimated from responses to the KCCQ and can facilitate cost-utility analysis from existing HF trials where only the KCCQ was administered. Future validation in other HF populations is warranted.</p>","PeriodicalId":36567,"journal":{"name":"MDM Policy and Practice","volume":"5 2","pages":"2381468320971606"},"PeriodicalIF":1.9000,"publicationDate":"2020-12-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1177/2381468320971606","citationCount":"1","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"MDM Policy and Practice","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2381468320971606","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2020/7/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 1
Abstract
Background. Health technology assessment bodies in several countries, including Japan and the United Kingdom, recommend mapping techniques to obtain utility scores in clinical trials that do not have a preference-based measure of health. This study sought to develop mapping algorithms to predict EQ-5D-3L scores from the Kansas City Cardiomyopathy Questionnaire (KCCQ) in patients with heart failure (HF). Methods. Data from the randomized, double-blind PARADIGM-HF trial were analyzed, and EQ-5D-3L scores were calculated using the Japanese and UK value sets. Several different model specifications were explored to best fit EQ-5D data collected at baseline with KCCQ scores, including ordinary least square regression, two-part, Tobit, and three-part models. Generalized estimating equations models were also fitted to analyze longitudinal EQ-5D data. To validate model predictions, the data set was split into a derivation (n = 4,465) from which the models were developed and a separate sample (n = 1,892) for validation. Results. There were only small differences between the different model classes tested. Model performance and predictive power was better for the item-level models than for the models including KCCQ domain scores. R2 statistics for the item-level models ranged from 0.45 to 0.52. Mean absolute error in the validation sample was 0.10 for the models using the Japanese value set and 0.114 for the UK models. All models showed some underprediction of utility above 0.75 and overprediction of utility below 0.5, but performed well for population-level estimates. Conclusions. Using data from a large clinical trial in HF, we found that EQ-5D-3L scores can be estimated from responses to the KCCQ and can facilitate cost-utility analysis from existing HF trials where only the KCCQ was administered. Future validation in other HF populations is warranted.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


