Judith Beschle, Michaela Döring, Christiane Kehrer, Christa Raabe, Ute Bayha, Manuel Strölin, Judith Böhringer, Andrea Bevot, Nadja Kaiser, Benjamin Bender, Alexander Grimm, Peter Lang, Ingo Müller, Ingeborg Krägeloh-Mann, Samuel Groeschel
{"title":"Early clinical course after hematopoietic stem cell transplantation in children with juvenile metachromatic leukodystrophy.","authors":"Judith Beschle, Michaela Döring, Christiane Kehrer, Christa Raabe, Ute Bayha, Manuel Strölin, Judith Böhringer, Andrea Bevot, Nadja Kaiser, Benjamin Bender, Alexander Grimm, Peter Lang, Ingo Müller, Ingeborg Krägeloh-Mann, Samuel Groeschel","doi":"10.1186/s40348-020-00103-7","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Long-term outcomes of hematopoietic stem cell transplantation (HSCT) in children with juvenile metachromatic leukodystrophy (MLD) have been investigated systematically, while short-term effects of HSCT on the course of the disease remain to be elucidated.</p><p><strong>Results: </strong>In this study, the clinical course was evaluated over the first 24 months following HSCT, conducted at our center in 12 children with juvenile MLD (mean follow-up 6.75 years, range 3-13.5) and compared with 35 non-transplanted children with juvenile MLD. Motor function (GMFM-88 and GMFC-MLD), cognitive function (FSIQ), peripheral neuropathy (tibial nerve conduction velocity), and cerebral changes (MLD-MR severity score) were tested prospectively. Seven children remained neurologically stable over a long period, five exhibited rapid disease progression over the first 12 to 18 months after transplantation. In the latter, time from first gross motor symptoms to loss of independent walking was significantly shorter compared with non-transplanted patients at the same stage of disease (p < 0.02). Positive prognostic factors were good motor function (GMFM = 100%, GMFC-MLD = 0) and a low MR severity score (≤ 17) at the time of HSCT.</p><p><strong>Conclusions: </strong>Our results show that if disease progression occurs, this happens early on after HSCT and proceeds faster than in non-transplanted children with juvenile MLD, indicating that HSCT may trigger disease progression.</p>","PeriodicalId":74215,"journal":{"name":"Molecular and cellular pediatrics","volume":"7 1","pages":"12"},"PeriodicalIF":3.4000,"publicationDate":"2020-09-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://sci-hub-pdf.com/10.1186/s40348-020-00103-7","citationCount":"17","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Molecular and cellular pediatrics","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40348-020-00103-7","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PEDIATRICS","Score":null,"Total":0}
引用次数: 17
Abstract
Background: Long-term outcomes of hematopoietic stem cell transplantation (HSCT) in children with juvenile metachromatic leukodystrophy (MLD) have been investigated systematically, while short-term effects of HSCT on the course of the disease remain to be elucidated.
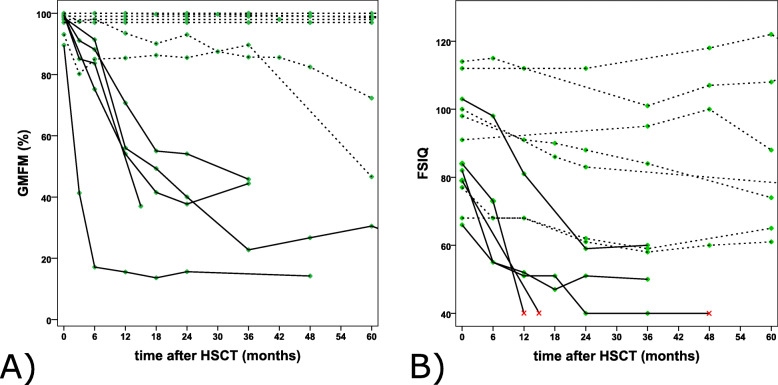
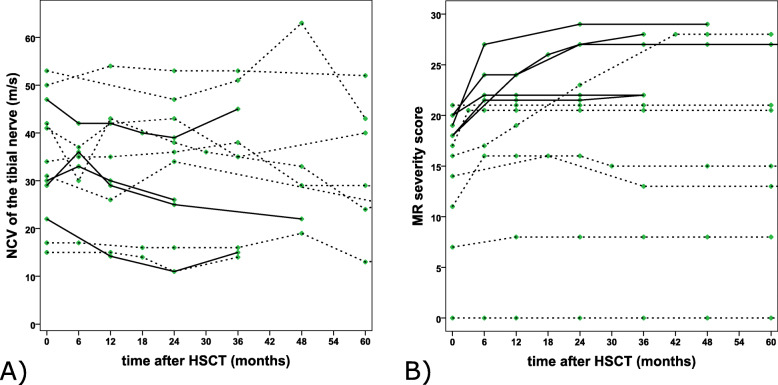
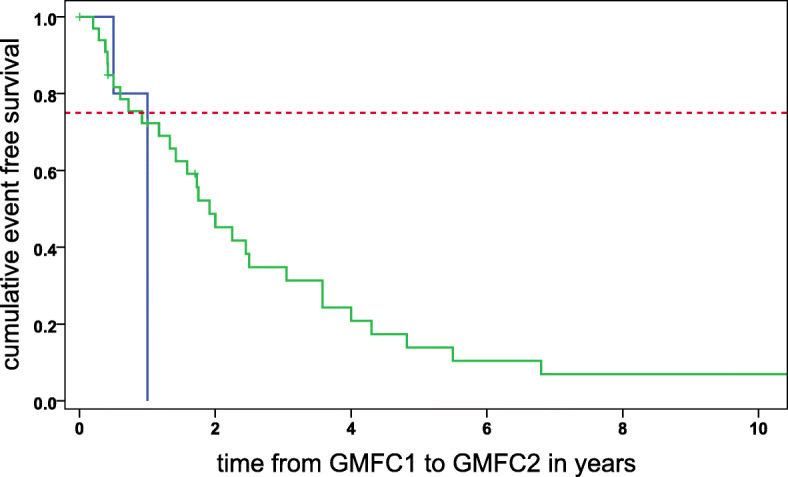
Results: In this study, the clinical course was evaluated over the first 24 months following HSCT, conducted at our center in 12 children with juvenile MLD (mean follow-up 6.75 years, range 3-13.5) and compared with 35 non-transplanted children with juvenile MLD. Motor function (GMFM-88 and GMFC-MLD), cognitive function (FSIQ), peripheral neuropathy (tibial nerve conduction velocity), and cerebral changes (MLD-MR severity score) were tested prospectively. Seven children remained neurologically stable over a long period, five exhibited rapid disease progression over the first 12 to 18 months after transplantation. In the latter, time from first gross motor symptoms to loss of independent walking was significantly shorter compared with non-transplanted patients at the same stage of disease (p < 0.02). Positive prognostic factors were good motor function (GMFM = 100%, GMFC-MLD = 0) and a low MR severity score (≤ 17) at the time of HSCT.
Conclusions: Our results show that if disease progression occurs, this happens early on after HSCT and proceeds faster than in non-transplanted children with juvenile MLD, indicating that HSCT may trigger disease progression.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


